GFR by Iohexol
Kindly download below document for the complete proposal as approved by the UCT Ethics Committee.
Kindly download below document for the complete proposal as approved by the UCT Ethics Committee.
| HOSP # | WARD | Nuclear Medicine | |
| CONSULTANT | DOB/AGE | 62 y Female |
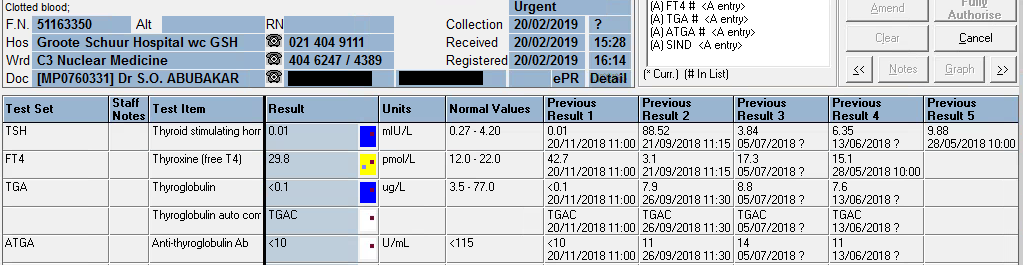
Thyroglobulin value of <0.1 ug/L upon signing results out.
Patient presented with a neck “swelling” in October 2016. Systemic complaints were not inquired, but none was reported.
TFT: euthyroid since presentation when the thyroid functions were first tested in 2016.
A solitary thyroid nodule was found in the neck, moving with swallowing.
TFT: euthyroid upon presentation, which is clear from the table below.
| 07/11/2019 | 08/08/2019 | 21/06/2019 | 20/02/2019 | 20/11/2018 | 26/09/2018 | 21/09/2018 | 05/07/2018 | 13/06/2018 | 29/05/2018 | 07/05/2018 | 08/01/2018 | 05/04/2017 | 26/10/2016 | |
| TSH | δ- 1,49 | δ- 7,07 H | δ+62,97 H | 0.01 L | δ- 0.01 L | δ+88,52 H | 3,84 | 6,35 H | δ+ 9,88 H | 2,86 | 4,05 | δ+ 3,26 | 1,62 | |
| Free T4 | 21,4 | δ+ 22,3 H | δ- 3.0 L | δ- 29,8 H | δ+ 42,7 H | δ- 3,1 L | 17,3 | CEGK | 15,1 | δ+ 14,9 | 12 | |||
| Free T3 | 4,8 | |||||||||||||
| Thyroglobulin (3.5-77.0 ug/L) | <0.1 L | <0.1 L | 0.1 L | <0.1 L | δ- <0.1 L | 7,9 | 8,8 | 7,6 | ||||||
| Anti-thyroglobulin Ab (<115 U/ml) | <10 | <10 | <10 | <10 | <10 | 11 | 14 | 11 |
From results above it can be seen that the patient was euthyroid upon presentation (in 2016 and later until excision – highlighted in bold)
Hemithyroidectomy was done in May 2018, and another hemithyroidectomy in September 2018, thus the thyroglobulin after the first and second surgery was still detectable, but absent after September 2018.
Ultrasound upon first presentation was indicative of a “suspicious nodule” in the thyroid gland.
PATHOLOGICAL DIAGNOSIS – excision biopsy of nodule (17/01/2018)
Specimen A:
Right lobe of thyroid, hemithryoidectomy:
Encapsulated follicular variant of papillary thyroid carcinoma
Specimen B:
Right cervical lymph node (Level VI), biopsy:
Negative for malignancy (0/1)
PATHOLOGICAL DIAGNOSIS – left thyroid lobectomy (11/05/2018):
Left lobe of thyroid, excision: Negative for malignancy
PATHOLOGICAL DIAGNOSIS:
Right thyroid, lobectomy: Negative for malignancy (05/09/2018):
The presence of thyroglobulin antibodies may interfere with the
thyroglobulin assay. The result of this test must be treated with reserve
if the patient has a positive thyroglobulin antibody test.TrakCare canned text for low thyroglobulin
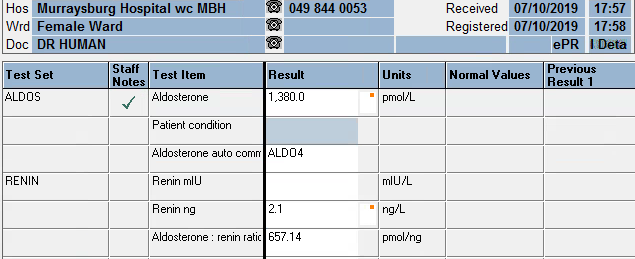
| HOSP # | WARD | Murraysburg Hospital, Female Ward | |
| CONSULTANT | DOB/AGE | 51 y female |
Aldosterone: 1380 pmol/L
Renin: 2.1 ng/L
Aldosterone: Renin ratio: 657.14 pmol/ng
Uncontrolled Hypertension, unresolved on maximum dose of 3 antihypertensives.




| Date | Sodium mmol/L | Potassium mmol/L | eGFR ml/min | GGT U/L | Chol mmol/L | TSH mIU/L | T4 pmol/L | FreeT3 pmol/L | Cort nmol/L |
| 21/04/2015 | 2,8 | >60 | 5,07 | ||||||
| 30/11/2015 | 3,8 | >60 | 4,53 | ||||||
| 15/11/2016 | >60 | 4,04 | |||||||
| 20/03/2017 | >60 | 4,36 | |||||||
| 05/06/2018 | 144 | 3,4 | 56 | 4,39 | 1,79 | 11,9 | 5 | 394 | |
| 20/08/2018 | 131 | 4,6 | 42 | ||||||
| 21/08/2018 | |||||||||
| 24/08/2018 | |||||||||
| 26/08/2018 | |||||||||
| 26/08/2018 | |||||||||
| 26/09/2019 | 139 | 2,4 | 45 | 0.81 | |||||
| 27/09/2019 | 142 | 2,6 | 43 | ||||||
| 01/10/2019 | |||||||||
| 02/10/2019 | 139 | 2,9 | 40 | CEGK | |||||
| 03/10/2019 | |||||||||
| 07/10/2019 | 138 | 3,9 | 38 | ||||||
| 31/10/2019 | 139 | 1,9 | 30 | 28 |
| Urine collection period | 24 h | Reference value |
| Urine volume | 3080 ml | |
| Ucreat | 2,2 mmol/L | |
| Umetadren | 160 nmol/L | |
| Unormetadren | 870 nmol/L | |
| dUmetadren | 493 nmol/24h | 152-913 |
| dUnormetadren | 2680 nmol/24h | 699-2643 |
| Umetadren:cr | 73 nmol/mmol creat | 17-91 |
| Unormetad:cr | 395 nmol/mmol creat | 75-309 |
Primary hyperaldosteronism causing secondary hypertension with accompanying renal injury.
Screening for primary hyperaldosteronism: most sensitive when >350 pmol/L
Beta-blockers suppress renin levels and should be stopped 2 weeks before testing.
Most sensitive when the ratio is >118 pmol/ng.