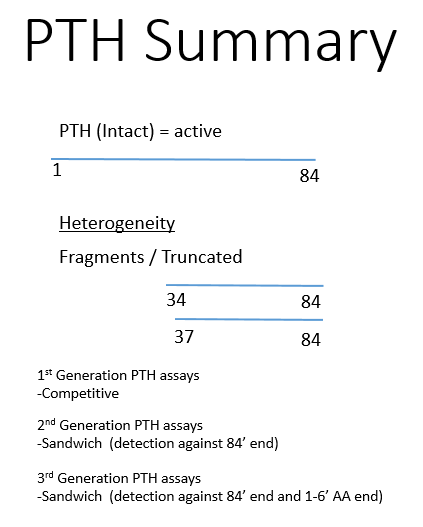
Dr. Jody Rusch’s simplistic explanation of PTH and its measurement
n-truncated are deficient in the first few aa’s (7-84) – hence biologically inactive.
1-11 aa sequence is necessary for function.
Different assays:
Intact PTH measurements: 7-84 and 1-84
Bioactive PTH: 1-84
CAP assay: cAMP inducible PTH. This assay determines the biologically active PTH by its ability to induce cAMP.
PTHrP assays and PTH assays are exclusive to each other by design.
A Case of Neurodevelopmental Delay
HOSP #
WARD
Neurodevelopmental clinic – Inkosi Albert Luthuli Hospital
CONSULTANT
Prof. George van der Watt
DOB/AGE
2y male
Abnormal Result
Urine organic acid analysis was performed upon which a big peak was seen, representative of phenylpyruvate.
Presenting Complaint
The patient was a 2 year old male evaluated at a neurology clinic for neurodevelopmental delay.
History
The patient’s brother died at 3 or 4 years of age with similar neurodevelopmental delay.
Examination
Unfortunately this information was unavailable. The clinician I got hold of at Inkosi Albert Luthuli hasn’t seen the patient himself.
Laboratory Investigations
Fig 1 – Urine organic acid screening by GCMS demonstrates elevations of the phenylketones: phenylpyruvate and 4-OH phenylpuyruvate. These findings are indicative of a diagnosis of phenylketonuria due to autosomal recessive deficiency of phenylalanine hydroxylase.
Other Investigations
The urine amino acid analysis yielded a significantly raised phenylalanine: 672 umol/L (ref <67)
Final Diagnosis
This is a case of phenylketonuria
The diagnosis is also supported by a plasma phenylalanine of 672 umol/L (ref < 67).
Take Home Messages
Build-up of phenylalanine gets metabolised to phenylpyruvate (which is seen in urine at high levels).
Phenylalanine levels >600 umol/L in serum is highly indicative of phenylketonuria
Prof. George van der Watt
Biopterin cycling defects usually cause levels >125 umol/L.
This deficiency is 4-monooxygenase deficiency.
Management of PKU is with a phenylalanine restricted diet.
Elevated anti-Thyroglobulin Antibodies
HOSP #
WARD
Oudtshoorn Clinic
CONSULTANT
George van der Watt & David Marais
DOB/AGE
66y Male
Abnormal Result
Presenting Complaint
Mr. X, a 66 year old male, complained of chest pain, was seen at the Oudtshoorn Emergency department and a myocardial infarction was excluded by three serial point-of-care (POC) Troponin I results.
History
Known with hypothyroidism, but the cause was not defined yet.
On Eltroxin 150 ug daily PO
No other treatment.
Various stool analyses had been sent in for culture, with no definitive result.
Examination
Unfortunately not known.
Laboratory Investigations
Free T4: 24.6 pmol/L (7.6 – 16.1 pmol/L)
Anti-Thyroglobulin Antibody levels were elevated at 1944 U/mL (ref. <115 U/mL).
Other Investigations
Later, by retrospective viewing of the patient’s results it was revealed:
Total Cholesterol (TC) was elevated at 7.6 mmol/L. Hypothyroidism is associated with hypercholesterolemia. It can be concluded by the retrospective overview of results that upon an episode of hypothyroidism, the patient had hypercholesterolemia. This was most likely due to cessation of Thyroxine treatment, to whatever reason.
Index sample marked by the yellow shade. TC result which is raised (upper left corner) corresponds to the severely hypothyroid episode as revealed by the low T4 on that same sample.
Investigations also confirmatory for auto-immune hypothyroidism are:
Anti-Thyroid peroxidase antibodies
Anti-TSH receptor antibodies
Final Diagnosis
Auto-immune hypothyroidism
Take Home Messages
Interestingly, numerous patients with hypothyroidism is diagnosed at our Lipid Clinic at Groote Schuur Hospital. Patients are being referred for hypercholesterolaemia. Generally referral to this clinic happens when TC > 7.5 mmol/L. These patients are referred as presumed to have familial hypercholesterolaemia, but upon further work-up it is found that many of these patients have long-standing untreated hypothyroidism.
Prevalences of antithyroid antibodies as summarized by Up-to-date: