Acute poisoning causing few to “fall flou”
| HOSP # | WARD | Casualties | |
| CONSULTANT | George van der Watt | DOB/AGE | 26 & 50 y/o males |
Abnormal Result
Urine toxicology screening / Urine organic acid analysis
Presenting Complaint
ESKOM load shedding resulted in failure of the power supply (including the emergency power generator) at a part of the hospital which included the routine toxicology screening lab at the Department of Pharmacology.
Two patient samples arrived at Red Cross Hospital IMD lab one Wednesday morning, brought personally by the Lab Manager of the Pharmacology Toxicology Department, requesting help to identify the cause of poisoning in two of six patients with alleged poisoning. At the time, the patients were both on ventilatory support in ICU due to depressed level of consciousness.
The repeated electricity power failures over a weekend, resulted in Toxicology’s state-of-the art tripple-quad tandem qTOF mass spectrometer to fail.
History
Six individuals were given a drink by a taxi driver in Landsdowne, Cape Town, on that Monday morning, all who collapsed few minutes later in the streets. Paramedics were on the scene soon and all affected patients were rushed to respective hospitals. See more on the Daily Voice.
Examination
The two individuals from whom we obtained urine for analysis, both had similar signs:
GCS was apparently 4/15, requiring intubation and ventilation.
Pupils were not miotic nor midriatic and signs were not in keeping with organophosphate poisoning.
Laboratory Investigations
No other laboratory investigations were available at the time. In retrospect, one of the patient’s results are available and serum electrolytes, liver enzymes, liver function and renal function tests were within normal range.
Other Investigations
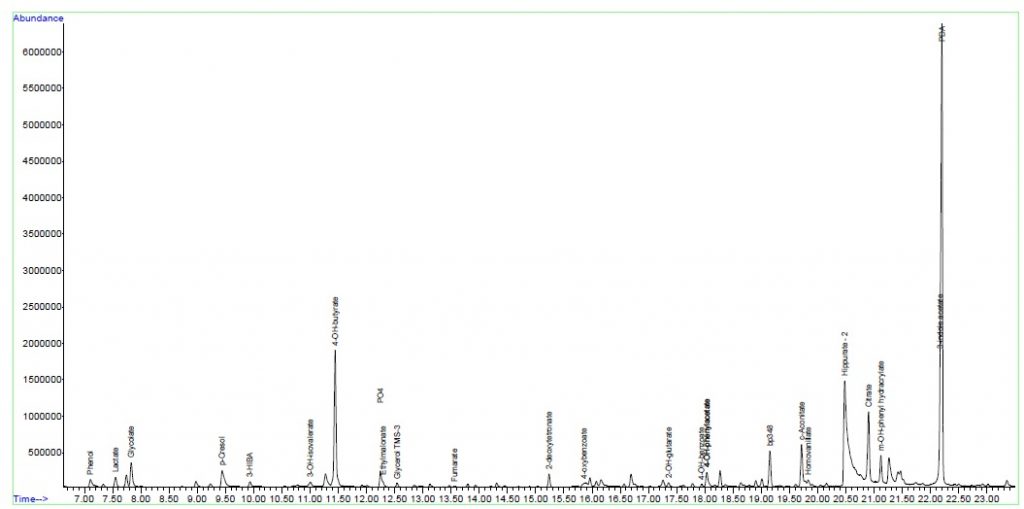
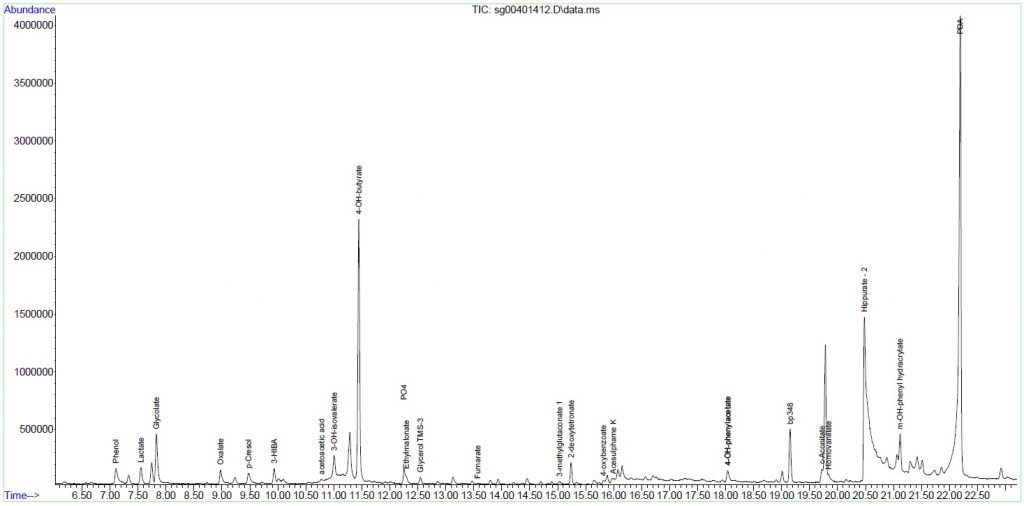
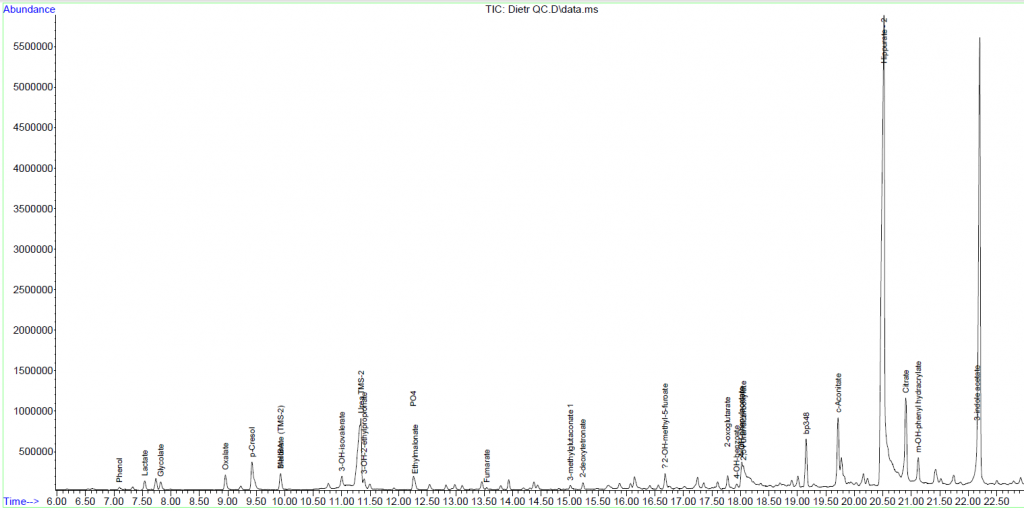
Urine organic acid analysis by GC-MS were done by us that day and we could identify Gamma-hydroxybutyrate (GHB) with an accurate hit to a known library adequately. We also ran a control urine sample of myself to prove the absence thereof as a negative control.
In the chromatograms below, note the height of the base peak, Pentadecanoic Acid (PDA) in relation to the peaks eluting at 11.45 minutes, 4-OH-butyrate, the analyte of interest. It can be seen that it is present in both the patient’s samples and is absent in the control sample.
Final Diagnosis
It was confirmed that both cases as analysed by us was in keeping with intoxication with 4-OH-butyrate (gammahydroxybutyrate; GHB).
Take Home Messages
We concluded that cases of gammahydroxybutyrate intoxication can be confirmed by urine GC-MS analysis at our IMD chemistry lab at Red Cross Children’s Hospital.
Gammahydroxybutyrate (GHB) has appeared to be quite a common (and perhaps re-emerging) drug in the Cape Town area. It can relatively easily be manufactured without sophisticated equipment and due to its ease of manufacture is not extensively made / traded by illicit drug traders.
GHB (an agonist of certain GABA receptors) can be manufactured relatively easily by addition of two ingredients, a prodrug gammabutyrolactone (GBL; a commercially available product) and an alkali hydroxide, such as sodium hydroxide to form GHB salt.
Other trade names of GHB include “Liquid Ecstasy”, “lollipops”, “Liquid X” or “Liquid E”.
See below a copy of the article as it appeared in the Daily Voice, a Cape Tonian newspaper:


