Hypocalcemia with Hypomagnesemia
| HOSP # | WARD | Internal Medicine ward | |
| CONSULTANT | George vd Watt / Heleen Vreede / David Marais | DOB/AGE | 58 y Male |
Abnormal Result
Upon signing out blood results:
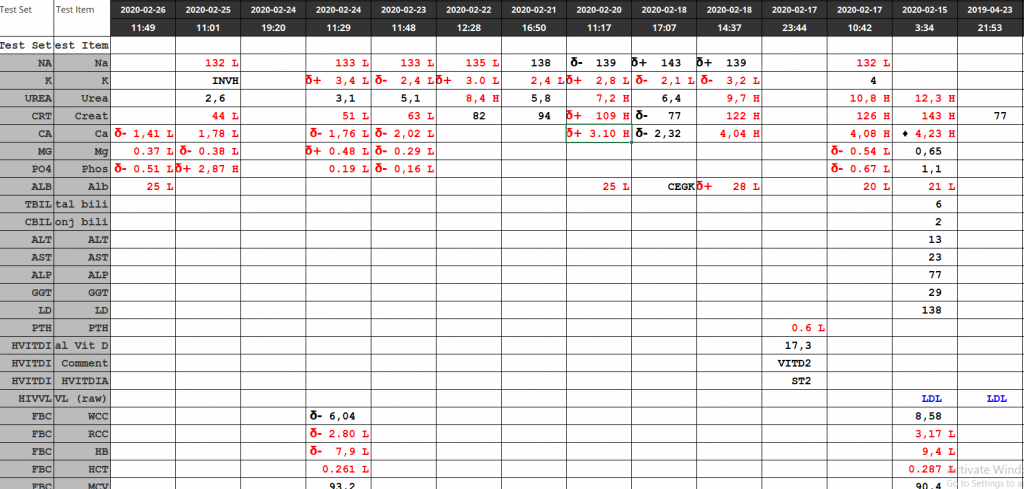
Calcium = 1.41 mmol/L – Critically low Calcium result
Magnesium = 0.37 mmol/L – Critically low Magnesium
Presenting Complaint
Loss of breath initially accompanied by weight loss.
Upon admission to the ward, patient was slightly delirious, but still able to walk and talk.
History
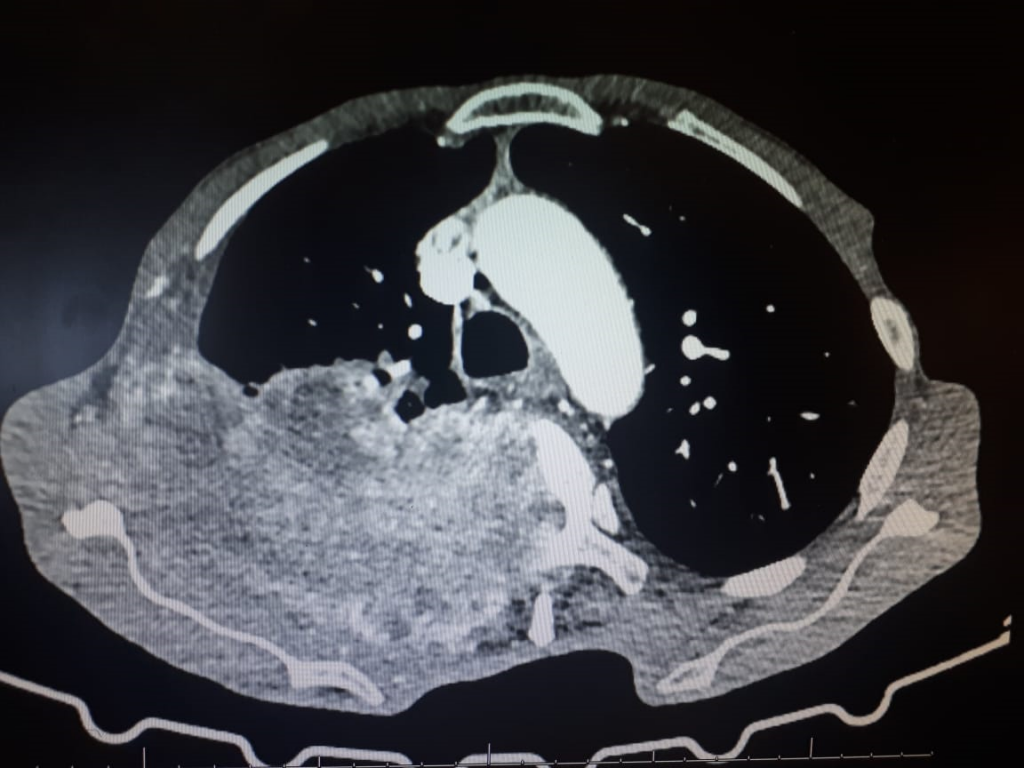
Patient with metastatic lung cancer and accompanying hypercalcemia, a week prior to the results as at present.
Doctor has given IV Bisphosphonate after the hypercalcemia was noted a week prior (Calcium = 4.23 mmol/L; Alb = 21 g/L; Corrected Ca = 4.61 mmol/L)
Examination
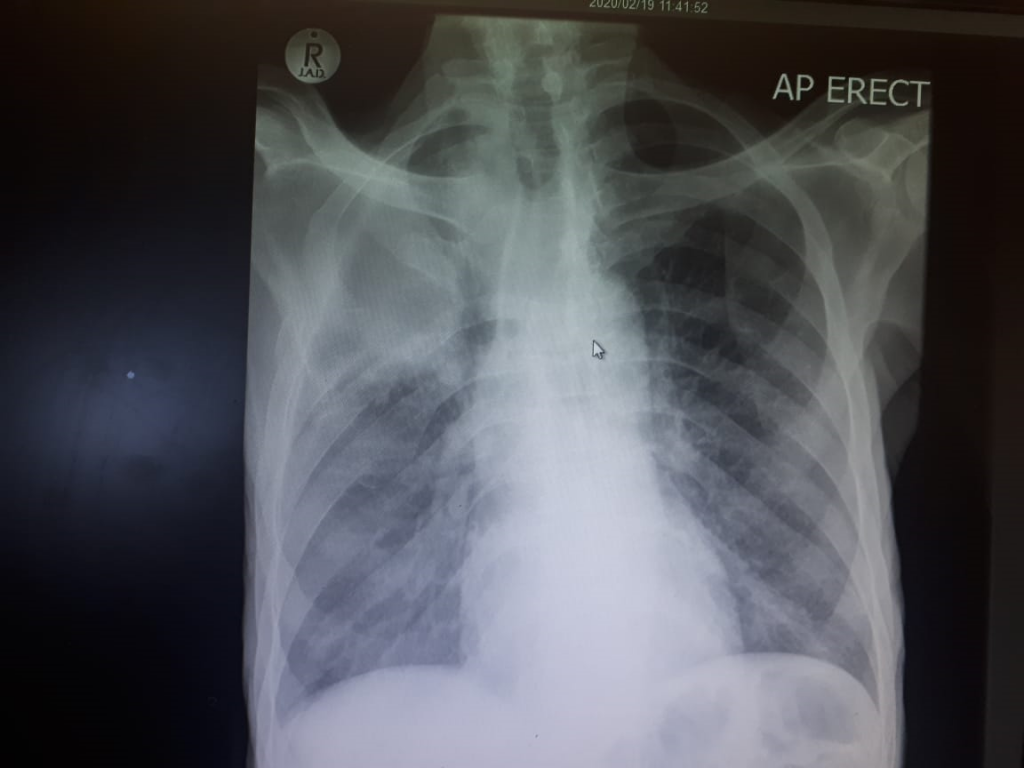
Extensive Crepitations over all the right lung fields.
Laboratory Investigations
Other Investigations
Final Diagnosis
Invasive lung CA with “hungry bones” after IV Zolendronic Acid
Vitamin D deficiency, preventing Calcium absorbtion after the Zolendronic acid started its action of inhibiting bone resorption.
Take Home Messages
CA causes hypercalcemia
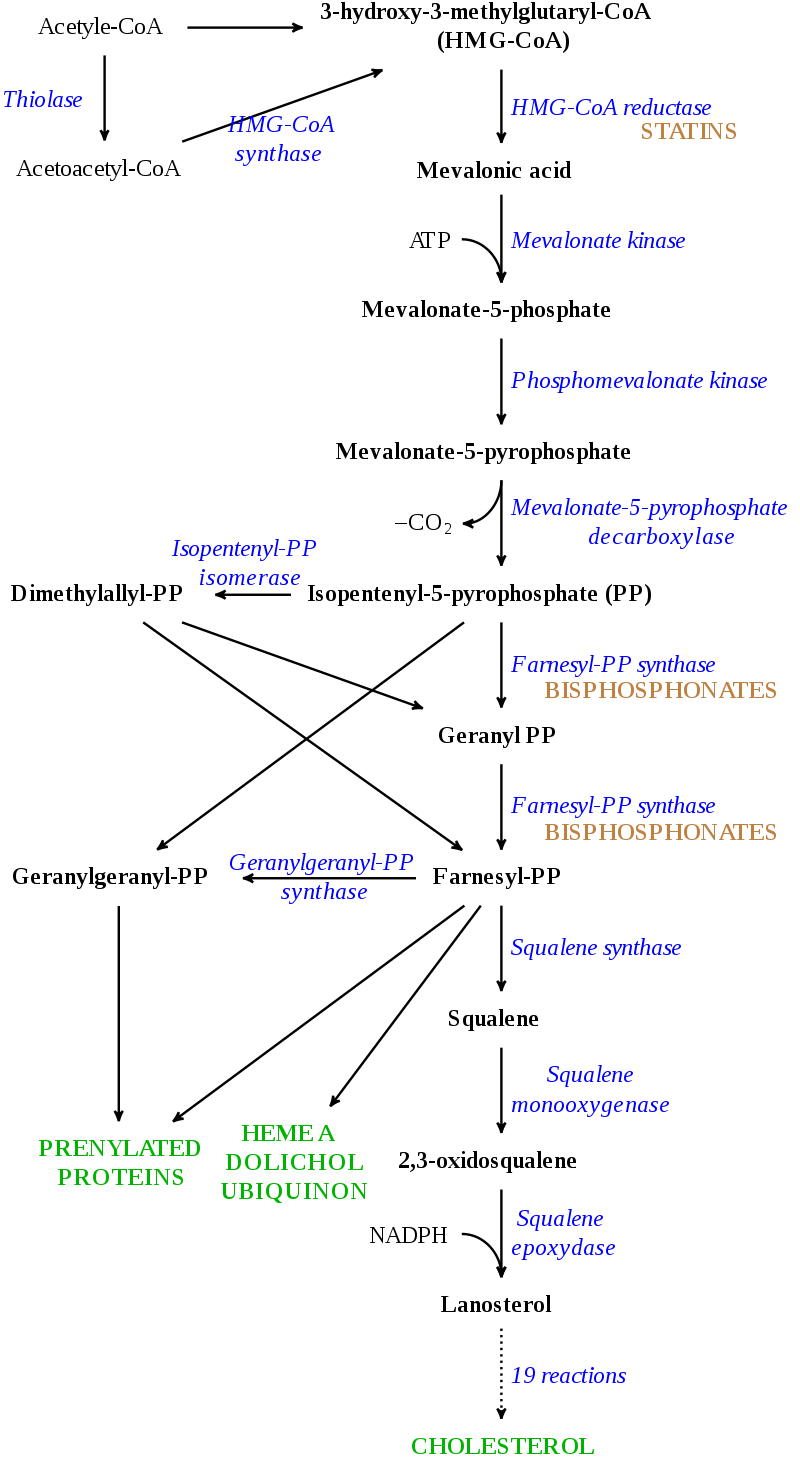
Bisphosphonates inhibits bone resorption. Because 99.95% of Ca in the body resides in bone, the effect in serum (the remaining 0.05% of total body Ca) can be significant.
All bisphosphonate drugs share a common phosphorus-carbon-phosphorus “backbone”:

They differ in the R-groups as above. It binds to calcium hydroxyapatite in bone.
Of the dose infused / absorbed, 50% is excreted unchanged by the kidney, the rest binds to bone tissue, where its elimination half life can apparently be up to 10 years! (UW Courses Web Server- https://courses.washington.edu/bonephys/opbis.html )
Because a bisphosphonate group mimics the structure of pyrophosphate, it can inhibit activation of enzymes that utilize pyrophosphate.
Magnesium follows Calcium levels, but Mg deficiency itself can also cause hypocalcemia.