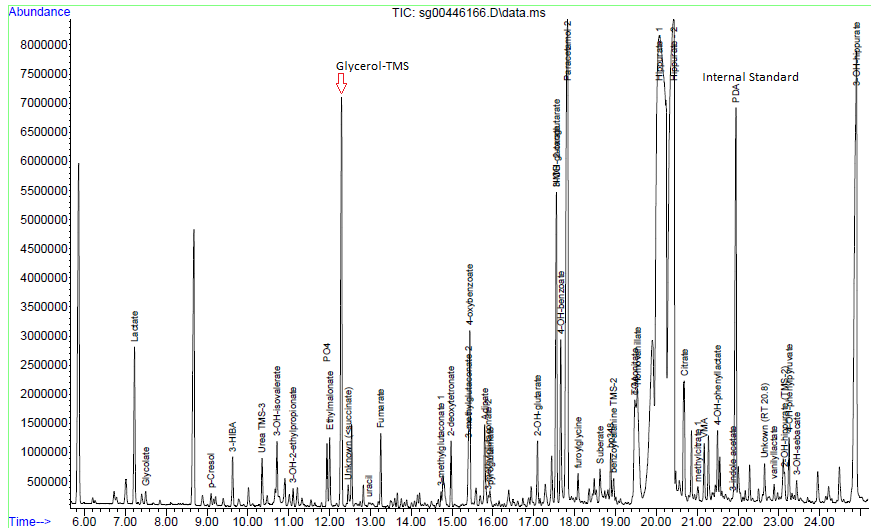
Glycerol which is significantly raised on urine organic acid analysis.
Figure 1 – Chromatogram. The high levels of Glycerol (with TMS – trimethyl silyl derivative) which is >0.5 the peak height of the internal standard (PCA – pentadecanoic acid).Figure 2 – Mass spectrum of the peak as indicated by Glycerol TMS above in Figure 1.Figure 3 – Follow up gas chromatogram without KY-jellyFigure 4 – Mass spectrum in the peak marked as “Glycerol-TMS” from figure 3.
Presenting Complaint
Patient is a 3 month old male with signs and symptoms of sepsis.
History
Patient presented with significant failure to thrive.
Laboratory Investigations
Triglycerides : 4.47 mmol/L
Other Investigations
Faecal elastase 81 ug/g stool
Reference range (adults and children > 1 month):
> 200 ug elastase/g stool: Normal exocrine pancreatic function
100-200 ug elastase/g stool: Moderate/mild pancreatic insufficiency
< 100 ug elastase/g stool: Severe exocrine pancreatic insufficiency
These ranges apply to formed stool samples. Watery stool samples may yield spuriously low elastase results due to dilution, and a formed stool sample should be sent for re-analysis.
Final Diagnosis
Glycerol contamination of the skin – as excluded by the repeat analysis.
Take Home Message
Glycerol (glycerine) is a common contaminant of urine organic acids due to being present in various skin products / creams. Contamination can be eliminated by thorough cleaning of the perineum with normal saline or doing an “in-out” catheterization procedure for urine collection in neonates. Interestingly glycerol is also one of the main ingredients in KY jelly, a common lubricant use for catheterization.
High glycerol in serum will present with a falsely high triglyceride level on most routine chemistry analysers due to the inherent enzymatic conversion of triglycerides to glycerol before further steps to measurement.
Figure 3 – Explanation of triglyceride determination by amperometric detection.
Sepsis is more common than inherited metabolic diseases and so is pre-analytical caveats such as glycerol contamination of the perineal skin.
Hyperaldosteronism with Hyperreninaemia in a 15 year old
The aldosterone:renin ratio (ARR) is a screening test for primary hyperaldosteronism and is most sensitive when both an absolute aldosterone > 350 pmol/L and an ARR > 118 pmol/ng is present.
Na: 138 mmol/L
K: 4.5 mmol/L
Urea 3.7 mmol/L
Creatinine: 49 umol/L
Total Calcium: 2.55 mmol/L
Urine dipstick 1+ protein
The urine protein:creatinine ratio was 0.044 g/mmol creat
Presenting Complaint
Patient presented with a 2 week history of blurry vision, intermittent headaches, hot flushes and mild intermittent epistaxis.
History
No known comorbidities
Multiple episodes of otitis media as a child
Presented with hypertension and evidence of target organ damage (retinopathy and left ventricular hypertrophy).
Funduscopy: Silver wiring, hard exudates, no haemorrhages, no papiloedema
CVS: bounding, peripherals pulses present. JVP raised, Undisplaced apex. Regular HR, no Radial/ femoral delays. Normal S1 & S2 with flowmurmur grade 2.
GIT: soft, non-tender. Ballotable left kidney, non-tender
Resp: Central Trachea, clear viscular breath sounds, no added sounds.
Neurological Exam: GCS 15/15, normal higher functions, no focal neurological signs.
BP control achieved with Doxazocin (increased to 4mg dly) and Atenolol (increased to 50mg dly)
Laboratory Investigations
TestItem
Value
Units
Reference Range
Urine collection period
24
hours
Urine volume
1280
mL
Urine metanephrine
350
nmol/L
Urine normetanephrine
16350
nmol/L
dU metanephrine
448
nmol/24 hrs
167 – 938
dU normetanephrine
20928 (High)
nmol/24 hrs
311 – 1562
Urine metanephrine : creat ratio
159 (High)
nmol/mmol creat
17 – 88
Urine normetanephrine : creat ratio
7432 (High)
nmol/mmol creat
23 – 176
Table 1 – Urine metanephrines (fractionated)
Other Investigations
ECG: Biatrial enlargement, left ventricular hypertrophy
Chest X-ray: Normal Cardio-thoracic index
Cardiac Ultrasound: Concentric left ventricular hypertrophy with preserved left ventricular ejection fraction. No valvular pathology.
KUB ultrasound: Similar kidney sizes. A mass with a cystic center was noted with no evidence of metastatic disease. Diagnosis suggested to be most likely a pheochromocytoma.
Final Diagnosis
Right-sided phaeochromocytoma
Take Home Message
Aldosterone : Renin ratio cannot be looked at alone. A raised value in either of the Aldosterone and Renin should be investigated further, especially if severely deranged like in this case.
Always investigate hypertension in a child until the cause is found. Hypertension in a child is not normal.
3 consecutive 24 hour urine collection samples are recommended for diagnosis of phaeochromocytoma as some tumours only secrete epinephrines / norepinephrines episodically. In this case however it was not necessary as the case was clear with a markedly raised dU-normetanephrine level.
Screening for pheochromocytoma is an essential part of the workup for secondary hypertension. Urinary vanillyl mandelic acid (VMA) was traditionally used to diagnose phaeochromocytoma. It has a low sensitivity (60-70%). Later, catecholamines measurement in plasma (PCAT) and urine (UCAT) emerged as useful tests. The sensitivity of catecholamines is limited by their episodic release from the tumour cells. The sensitivity ranges from 76-86 % for PCAT and UCAT and the specificity is around 81-99 %.
Metanephrines are methylated metabolites of catecholamines.
Metanephrines are secreted continuously from the tumour cells, independent of the intermittent release of catecholamines. The metanephrines are metabolized by conjugation, primarily in the hepatomesentric organs. Plasma metanephrines (pMN) are measured in the free form (not routinely offered in South Africa) whereas urinary metanephrines (uMN) represent mainly the conjugated form. Hence compared to pMN, uMN is less specific. Studies have shown that plasma free metanephrines have a sensitivity of 96-100 per cent and specificity of 85-100 % superior to that of uMN which has a sensitivity of 93-99.6 per cent and specificity of 71-77 per cent.
Previous methods used colorimetry or spectrophotometry as total MET (metanephrine + normetanephrines) which includes a combined measurement of metanephrine (MN) and normetanephrine (NMN). These methods were superseded by liquid chromatographic assays (LC) that allow individual measurement of MN and NMN.
At Red Cross Hospital Laboratory we use a gas chromatography with mass spectrometry, which is not so widely used for fractionated metanephrines. An isotope dilution method is employed, bringing the method up to internationally recognized standards and the quality assurance of the method at the Red Cross Chemistry lab performs well on the international EQA scheme used.