A case of raised PSA with ALP
| HOSP # | Lab no. SA04016354 | WARD | Orthopaedic Clinic |
| CONSULTANT | Jody Rusch | DOB/AGE | 61y Male |
Abnormal Result
PSA: 846.5 ug/L
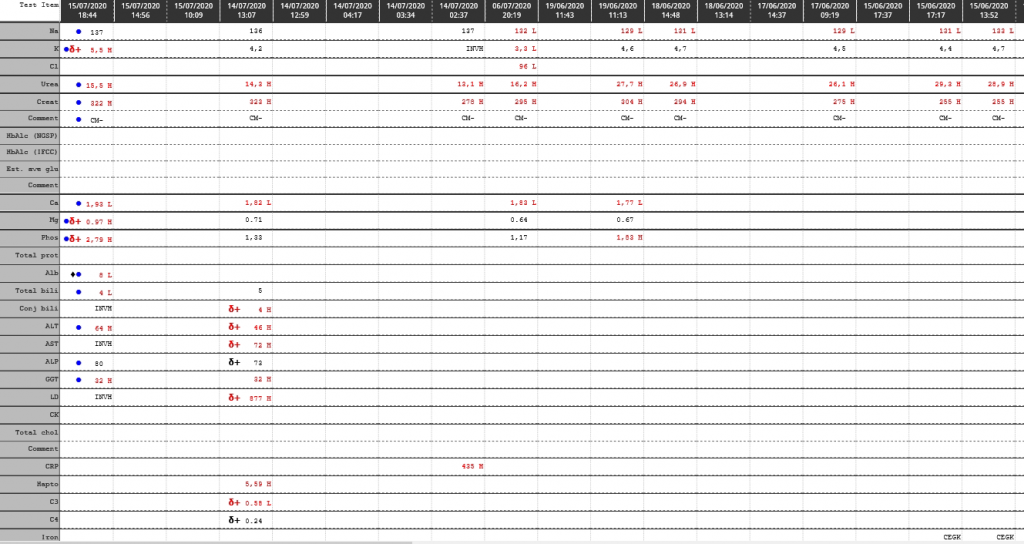
ALP: 284 U/L (53 – 128)
Presenting Complaint
Painful ”lumps” in groin + constipation
Spine pain
History
Smoker (>45 years)
No other co-morbidities
6/12 history of generalized body pain (mostly spine)
Red Flags (weightloss, night pain not responding to analgesia)
Examination
O/E: Pallor (Hb 8.6), Wasted. Clinically painful bilateral inguinal lymph nodes PR: normal tone, no masses, no blood, prostate smooth
Laboratory Investigations
| Na | 138 mM |
| K | 4,7 mM |
| Cl | 101 mM |
| Urea | 10,3 mM |
| Creat | 69 uM |
| eGFR by MDRD | >60 ml/min/m2 |
| eGFR by CKDEPI | 97 ml/min/m2 |
| Ca | 2,26 mmol/L |
| Mg | 1,03 mmol/L |
| Phos | 1,01 mmol/L |
| Total prot | 73 g/L |
| Alb | 37 g/L |
| Total bili | 3 umol/L |
| Conj bili | 2 umol/L |
| ALT | 15 U/L (10-40) |
| AST | 19 U/L (15-40) |
| ALP | 284 U/L (53 – 128) |
| GGT | 76 U/L (<68) |
| LD | 345 U/L |
| CRP | 52 mg/L (<10) |
| Total PSA | 846.5 ug/L (<4) |
| TSH | 1,33 mIU/L (0.27 – 4.2) |
| Hb | 5.6 g/dL |
| MCV | 88.3 fL |
| WCC | 7.57 cells/uL |
Other Investigations
Chest X-Ray: Left hilar opacities
X-ray of the limbs: Global lytic lesions involving both proximal femurs





Prostate biopsy
- MACROSCOPY: Specimen consists of two cores, the longest measuring 12mm in length.
- MICROSCOPY Sections show 2 prostatic cores, both infiltrated by a prostatic adenocarcinoma.
- % Ca core 1: 90%
- % Ca core 2: 60%
- Gleason score: 5 + 4
- Grade group: 5
- High grade PIN: Not seen
- Seminal vesicle: Not seen
- Perineural invasion: Present
- Fat (extraprostatic) involvement: Not seen
- PATHOLOGICAL DIAGNOSIS:
- Prostate, needle biopsy: Prostatic acinar adenocarcinoma
Final Diagnosis
Metastatic Prostate Carcinoma with multiple metastases to the bones (thoracic spine and both femurs).
Take Home Message
Prostate-specific antigen (PSA, also known as kallikrein III, seminin, semenogelase, γ-seminoprotein and P-30 antigen) is a 34-kD glycoprotein produced almost exclusively by the prostate gland. It is a serine protease enzyme.
Most PSA in the blood is bound to serum proteins. A small amount is not protein-bound and is called ‘free PSA’. In men with prostate cancer, the ratio of free (unbound) PSA to total PSA is decreased. The risk of cancer increases if the free to total ratio is less than 25%.
The lower the ratio is, the greater the probability of prostate cancer. Measuring the ratio of free to total PSA appears to be particularly promising for eliminating unnecessary biopsies in men with PSA levels between 4 and 10 mg/L.
ALP (alkaline phosphatase) is well known to be a marker of ductal hepatic damage. ALP, being an isozyme, however has its origin from various tissue sources in the body. It is present in the liver, bile duct, kidney, bone, intestinal mucosa and placenta. The majority of ALP in serum is from either skeletal or liver origin. In adults the major form is from liver and in children the major form is from the skeleton.
Blood levels of alkaline phosphatase increase by two to four times during pregnancy. This is a result of additional alkaline phosphatase produced by the placenta.
If it is unclear why alkaline phosphatase is elevated, isoenzyme studies using electrophoresis can confirm the source of the ALP. It would likely in this patient be quite clear that the raised ALP would be due to the excess leakage from the osteolitic lesions from the metastases, but who knows, the patient may have had a beer or five in the preceding 3 weeks leading up to the bloods being drawn. The fact that the other liver enzymes are near-normal, makes alcohol consumption less likely though.