Bicarbonate HCO3 CO2 CO3
Method
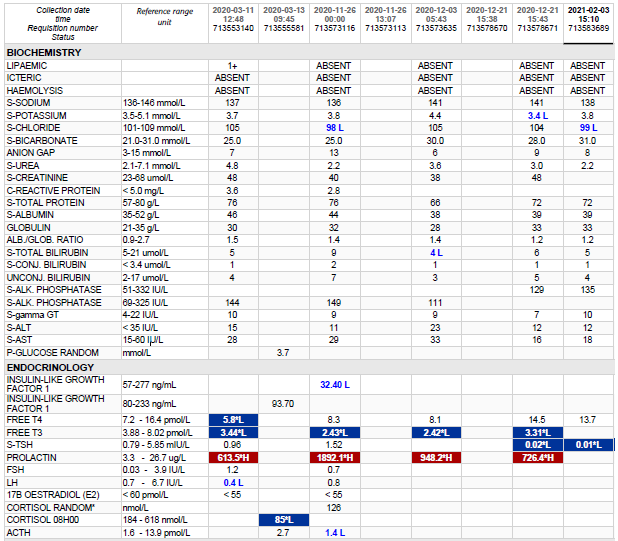
Bicarbonate is the second largest fraction of the anions in plasma. Included in this fraction are the bicarbonate (HCO3–) and carbonate (CO32-) ions, as well as the carbamino compounds. At the physiological pH of blood, the concentration of carbonate is 1/1000 that of bicarbonate. The carbamino compounds are also present in such low quantities that they are generally not mentioned specifically.
Several different methods for the determination of bicarbonate in serum and plasma have been reported. Most of these procedures utilize acidification of the sample and conversion of all carbon dioxide forms to CO2 gas. The amount of gas formed is measured by manometric or volumetric devices, ion selective electrodes, or spectrophotometric techniques. These methods are either cumbersome, time-consuming, technique-oriented, and/or require special equipment.
Enzymatic procedures using phosphoenolpyruvate carboxylase (PEPC) have been described.
The bicarbonate content of serum or plasma is a significant indicator of electrolyte dispersion and anion deficit. Together with pH determination, bicarbonate measurements are used in the diagnosis and treatment of numerous potentially serious disorders associated with acid-base imbalance in the respiratory and metabolic systems.
Test principle
Bicarbonate reacts with phosphoenolpyruvate (PEP) in the presence of PEPC to produce oxaloacetate and phosphate:
PEPC
PEP + HCO3– —> oxaloacetate + H2PO4–
The above reaction is coupled with one involving the transfer of a hydrogen ion from NADH analog to oxaloacetate using MDH.
MDH
Oxaloacetate + NADH analog + H+ —> malate + NAD+ analog
The resultant consumption of NADH analog causes a decrease in absorbance, which is proportional to the concentration of bicarbonate in the sample being assayed.