Section 2 – Candidate Details
General details
| SA ID: 9110245133085 HPCSA number: MP 0801186 Trainee #: C17-01-04 |
dieter.vdwesthuizen@nhls.ac.za / dietervdwes@gmail.com Tel (w): 021 404 4135 Tel (m): 082 861 2093 |
| Work Address: C20 NHLS Laboratory, Groote Schuur Hospital, Main Road, Observatory, Cape Town, 7925 |
Residential Address: 2 Brunswick Road, Tamboerskloof, Cape Town, 8001 |
Qualifications
Degrees
| Dec 2014 | M.B.Ch.B. | University of the Free State, South Africa |
Diplomas
| Jan 2015 | Basic Life Support | University of the Free State, South Africa |
Short Courses
| Sept 2017 | Marketing Course (10 weeks) | University of Cape Town (via Getsmarter) |
| April 2019 | STATA basic data analysis(3 days) | Centre for Statistical Analysis and Research: CESAR |
Hospital Appointments
| Jan 2018 – Current | Registrar in Chemical Pathology | NHLS, Groote Schuur Hospital & Red Cross Children’s Hospital |
| Jan 2017 – Dec 2017 | Community Service | Policlinic OPD (Area Military Health Unit) & 3 Military Hospital, Bloemfontein, South Africa |
| Jan 2015 – Dec 2016 | Medical Internship | Pelonomi, Universitas & National Hospitals, Free State Hospital Complex, Bloemfontein, South Africa |
Section 2.1 – Portfolio of Learning
A possible case of growth hormone deficiency
| HOSP # | WARD | G4 Adolescent Ward | |
| CONSULTANT | Ariane Spitaels / Heleen Vreede | DOB/AGE | 12 y Male |
Abnormal Result
Low growth hormone with an abnormal clonidine stimulation test.
Presenting Complaint
At 7 years of age, patient presented with chronic headaches.
History
CT-brain revealed acute hydrocephalus. Endoscopic 3rd ventriculostomy was done. MRI revealed a lesion posterior to mid-brain and pons as well as a hyper-intensity on T1 with contrast. A glioma was queried as the cause.
Patient recently was identified to have decreased growth velocity (4cm / year) in the preceding 6 months and was also admitted for a clonidine stimulation test. Patient was primed for 2 days.
Examination
N/A
Laboratory Investigations
Histology
GROSS DESCRIPTION: Specimen labelled Sub-occipital tumour consists of 5 fragments of tissue measuring 4-5mm each.
HISTOLOGY: Sections of the brain biopsies show sheets of bipolar neoplastic cells with piloid cytoplasmic processes. Scattered pleomorphic tumour cells, microcystic areas and areas resembling oligodendrocytes are present. Rosenthal fibres and eosinophilic granular bodies are not a prominent feature. There is no vascular proliferation or tumour necrosis.
Comment: See frozen section below.
PARAFFIN SECTIONS: Sections of the brain tumour show piloid areas (cells with hair-like processes, gemistocytic cells and focal Rosenthal fibres. Mild nuclear atypia is noted. There are no mitotic figures, vascular proliferation or areas of necrosis. Scattered entrapped neurons are noted.
IMMUNNOHISTOCHEMISTRY: Neurofilament: Highlight background neural processes
GFAP: Diffusely positive p53: Weak staining in less than 10% of the tumour cells, interpreted as negative.
Ki67 proliferation index: < 4%
CONCLUSION: Brain, biopsy: Juvenile pilocytic astrocytoma.
Other Investigations
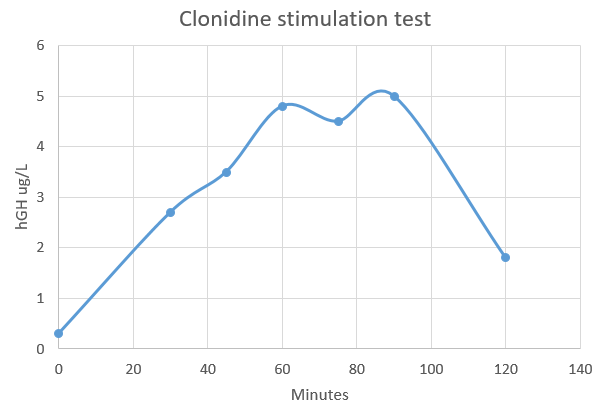
Clonidine stimulation testing
| Time after Clonidine injection (minutes) | Result |
| 0 | 0.3 |
| 30 | 2.7 |
| 45 | 3.5 |
| 60 | 4.8 |
| 75 | 4.5 |
| 90 | 5 |
| 120 | 1.8 |
Final Diagnosis
Since the hGH concentration did not rise to above 10 ug/L, the diagnosis is likely that of growth hormone deficiency, or hyposomatotropism.
Take Home Message
Provocative Testing for Growth Hormone deficiency (GHD)
The following provocative (dynamic) tests are available for hGH deficiency:
- Insulin tolerance test
- Clonidine stimulation test
- Levodopa-propranolol HCl test
- Arginine HCl test
- Glucagon test
Provocative GH testing is criticized for several reasons, including the following:
- None of the tests reproduces the physiologic secretory pattern of GH because they involve the use of pharmacologic stimuli to indirectly assess physiologic GH production.
- Individual clinicians assign what are essentially arbitrary definitions for subnormal responses (ie. cutoffs for peak serum GH values)
- The reproducibility of provocative tests and GH RIAs is limited. Many pediatric endocrinologists apply other clinical criteria (eg, growth velocity Z score below -2) and do not perform provocative GH tests to diagnose GHD.
Despite limitations, provocative GH tests remain helpful ways to measure GH reserve. Pediatric endocrinologists use physiologic stimuli (eg, strenuous exercise, fasting, deep sleep) and pharmacologic stimuli (eg, clonidine, levodopa-propranolol, glucagon, arginine, insulin) to provoke GH secretion. The tests must be performed after overnight fasting, firstly ensuring that the children are euthytoid.
To improve diagnostic sensitivity and specificity, at least 2 provocative tests are performed. Immediately before and during the earliest phases of puberty, GH production is often indistinguishable in unaffected children and in children with GHD. Serum GH concentrations typically rise during puberty. Many investigators suggest that children approaching puberty should be given gonadal steroids to prime the growth hormone-releasing hormone (GHRH)-GH axis before testing.
Most clinicians use a peak serum GH concentration of more than 10 ng/mL (30 IU) to exclude GHD in children. Specific provocative tests are described below.
Insulin tolerance test
Insulin-induced hypoglycemia is the most potent stimulus for GH secretion and the most dangerous tool for provocative GH testing in patients who may have GH deficiency. Insulin tolerance testing takes advantage of the hormonal counterregulatory response to hypoglycemia. In patients without GHD, plasma concentrations of glucagon, epinephrine, norepinephrine, cortisol, corticotropin, and GH are elevated in response to acute hypoglycemia.
To perform the test, patients fast for 8 hours. Then, lispro insulin 0.1 U/kg of body weight is administered rapidly as an intravenous bolus. Serial blood samples are subsequently obtained to measure GH, cortisol, and glucose concentrations at 0, 15, 30, 60, 75, 90, and 120 minutes. With each sample, the blood glucose level is simultaneously determined by using a bedside glucometer to document an appropriate reduction and to ensure safety. Performance of the test is considered adequate when the blood glucose level decreases below 50% of its baseline value.
Adverse effects expected during the procedure include symptoms secondary to hypoglycemia, such as lethargy, shaking, confusion, headache, abdominal pain, nausea, vomiting, syncope, and seizure activity. The test must be performed under the watchful eye of the physician who can begin prompt resuscitation with glucose and/or glucagon as soon as the diagnostic samples have been obtained. To date, the insulin tolerance test is the only provocative test associated with fatalities; therefore, personnel must be trained and conduct the test judiciously.
Clonidine stimulation test
Clonidine acts centrally to stimulate alpha-adrenergic receptors, which are involved in regulating GH release. Serum GH levels are obtained at baseline and at 60 minutes and 90 minutes after the oral administration of clonidine 0.1 mg/kg. Clonidine may induce hypotension during the test. Therefore, warn parents that they may experience lethargy and/or depression for 24 hours after clonidine is administered.
Levodopa-propranolol HCl test
Levodopa is a dopamine receptor agonist. Dopamine is involved in the stimulation of GH secretion. In the converse, beta-adrenergic control negatively regulates GH release.
Propranolol is a beta-blocker used to hinder inhibitory input affecting GH release, while levodopa simultaneously stimulates GH release by means of the dopaminergic pathway. Propranolol 0.75-1 mg/kg is orally administered before levodopa. The dosage of levodopa for levodopa-propranolol HCl testing varies with weight, so that children weighing less than 15 kg receive 125 mg, children weighing 10-30 kg receive 250 mg, and children weighing more than 30 kg receive 500 mg.
Blood samples for GH testing are drawn at 0, 60, and 90 minutes after the administration of levodopa. Adverse effects include nausea and, in rare cases, emesis. In addition, the patient’s heart rate may decrease because of the use of propranolol. Closely monitor his or her vital signs, and ensure that appropriate resuscitative measures are available.
Arginine HCl test
Arginine appears to exert a direct depolarizing action on somatropic neurons, increasing GH secretion. After an overnight fast, patients are given 10% arginine HCl in 0.9% NaCl 0.5 g/kg (not to exceed 30 g) as a constant intravenous infusion over 30 minutes. Blood samples for GH testing are obtained at 0, 15, 30, 45, and 60 minutes after the infusion of arginine is begun. Arginine has historically been used as a primer before insulin is administered during insulin tolerance testing.
Glucagon test
Glucagon increases peripheral glucose concentrations by means of glycogenolysis and gluconeogenesis. Because glucagon is rapidly metabolized, an abrupt reduction in serum glucose concentration ensues and triggers the release of counterregulatory hormones.
After fasting overnight, patients receive an intramuscular injection of glucagon 0.03 mg/kg (not to exceed 1 mg). Some clinicians advocate the concomitant use of propranolol to inhibit the catecholaminergic response to hypoglycemia. Serum GH concentrations are determined at 0, 30, 60, 90, 120, 150, and 180 minutes after glucagon administration. Nausea and, occasionally, emesis may occur.
Growth hormone reference intervals provided should be seen as a guideline only. Specifically, reference intervals or random growth hormone levels are not useful for diagnosing growth hormone deficiency.
For this, stimulation tests are required. A recent paper established clinical evidence-based cut-off limits for
diagnosing growth hormone deficiency in children and adolescents following growth hormone stimulation tests, by various commercially available immunoassays, compared to isotope dilution mass spectrometry (ID-MS).
Reference: Clinical evidence-based cutoff limits for GH stimulation tests in children with a backup of results with reference to mass spectrometry, Wagner et al, European Journal of Endocrinology (2014)171, 389-397TrakCare Autocomment
| Assay | Cut-off limit |
| Immulite 2000 (Siemens) | 7.77 ug/L |
| AutoDELFIA (Perkin-Elmer) | 7.44 ug/L |
| iSYS (Immunodiagnostic System) | 7.09 ug/L |
| Liaison (DiaSorin) | 6.25 ug/L <– Current assay |
| DXI (Beckman-Coulter) | 5.15 ug/L |
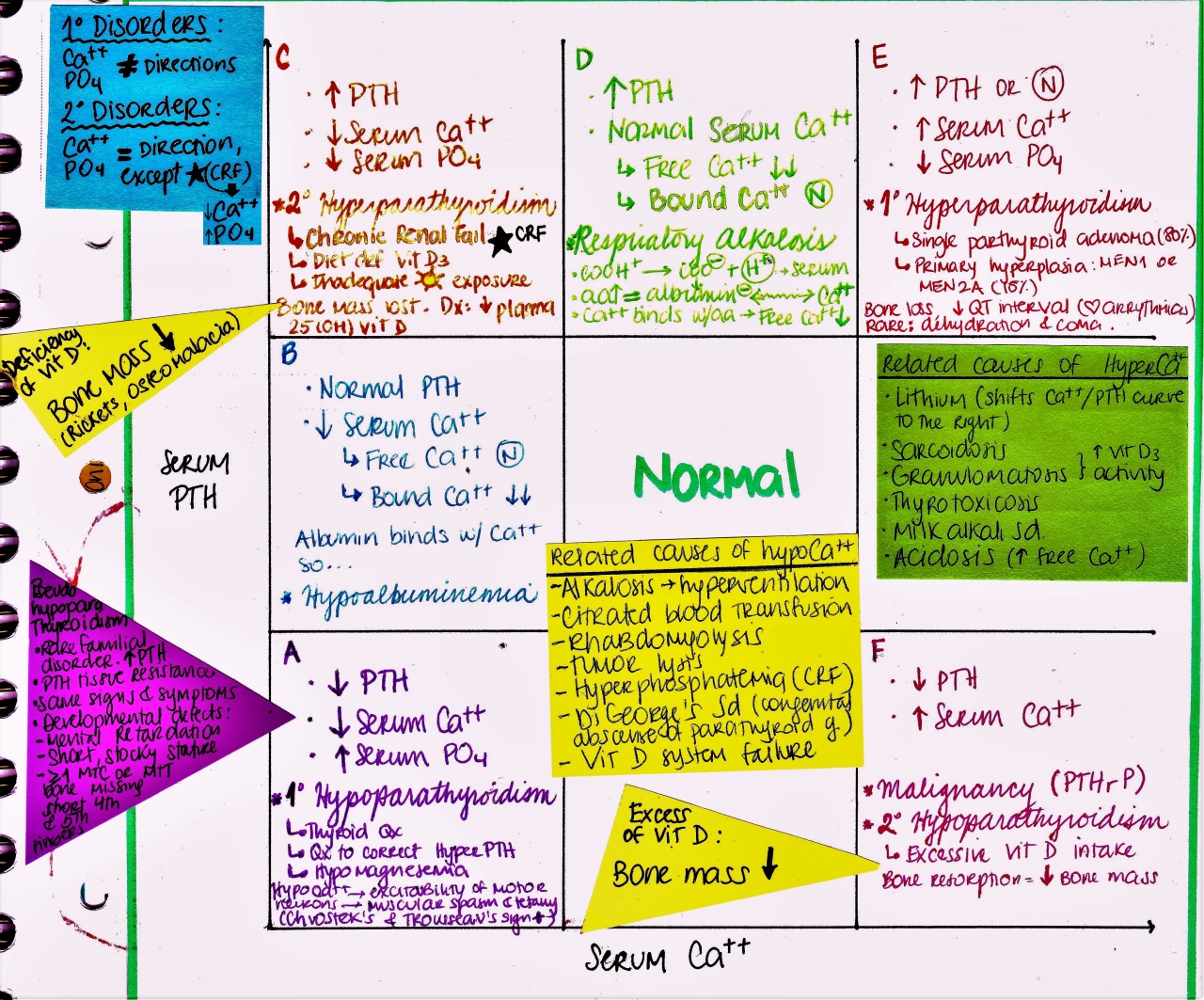
A case of Primary hyperparathyroidism and subsequent parathyroidectomy
| HOSP # | WARD | Medical Ward | |
| CONSULTANT | Dr. Jody Rusch | DOB/AGE | 59 Y Male |
Abnormal Result
Hypercalcemia with hypophosphatemia
Presenting Complaint
History
This is a patient with parathyroid adenoma (and resulting longstanding hypercalcemia and hypophosphatemia, which is typical). Adenoma was removed yesterday, acc. to what I can see on a frozen section. Phosphate is dropping even more 0.42 mM (0.78 – 1.42) (on bloods taken this afternoon) and it will likely become significantly lower even.
Examination
Laboratory Investigations

PTH was initially significantly raised, although the renal function was normal. This means that there is likely hypercalcemia due to primary hyperparathyroidism.

Other Investigations
Final Diagnosis
Take Home Message
Phosphate supplementation may be quite important as there was longstanding autonomous PTH secretion, depleting stores of phosphate via phosphaturia (also PTH induced). There will likely not be much PTH secretion for some while, hence Vit. D activation will seize and little phosphate absorbed from the GIT due to longstanding lack of phosphate transporters. FGF-23 secretion will also seize and with the lack of PTH, the bone will not resorb and the remodeling process will consume the phosphate in the blood. Most mechanisms to increase phosphate physiologically will likely be dysfunctional at this time. Because he will not adequately absorb phosphate from the GIT (because of failure to activate Vit. D, he may need supplementation of phosphate IV).
Kidneys will however be a bit less phosphaturic (due to lack of PTH), thus he may respond quite well to IV phosphate.
A case of abnormal CSF chemistry results

| HOSP # | WARD | Neurology Ward | |
| CONSULTANT | Jody Rusch | DOB/AGE | 17 y Female |
Abnormal Result
Increased CSF IgG / albumin Index
Decreased CSF Glucose
Presenting Complaint
At this admission, she presented to Groote Schuur Hospital with a history of parasthesias and lower limb weakness. Her symptoms have had a rapid progression to completed paraplegia, with loss of sphincter control over three days. She does not report altered sensorium or alteration in her sleep wake cycle.
History
The patient had two prior episodes of TB and Systemic Lupus Erythematosis, which was diagnosed in 2017. Her presenting symptoms was malar rash, arthralgia, and having positive serological markers.
She has subsequently been diagnosed with class-II nephritis and autoimmune haemolytic anaemia. She was on maintenance immunosuppression regimen of prednisone and azathioprine between 2017-19.
She has had two prior episodes of TB in 2014 and 2018.
She was diagnosed with optic neuritis in October 2019, after she developed visual loss in her left eye with no perception of light. Retrospectively she reports a prior episode of unilateral visual loss in her right eye in February 2019, consistent with an episode of ON. On the basis of her ON she had her immunosuppression escalated to monthly pulses of cyclophosphamide, from November 2019 until march 2020.
She has now developed an acute severe inflammatory longitudinally extensive myelitis, as result of seropositive Neuromyelitis Optica Spectrum Disorder (NMOSD).
Neuromyelitis Optica Spectrum Disorder, or NMOSD, is a rare, lifelong and debilitating autoimmune disease of the central nervous system (CNS), characterized by inflammation in the optic nerve and spinal cord.
Examination
Higher function examination was normal. Cranial nerve examination revealed bilaterally dilated pupils with sluggish responses. Relative afferent pupillary defect (RAPD) was noted in the left eye. Visual acquity is reduced in both eyes, with the left being more severely affected than the right. Fundoscopy showed bilateral disc pallor, no active papillitis. She had no further cranial nerve or bulbar signs. Upper limb motor examination showed paratonia in the right upper limb. The left had mild loss of dexterity and power in her left hand. Reflexes were symmetrical. Power in her lower limbs was reduced with 0/5 power, she would have intermittent involuntary movements to tactile stimuli. She was hypertonic with a triple response. She has a T4 sensory level to light touch and pin prick and has marked joint position sensation loss in both her legs.
The patient was admitted for evaluation of her Myelitis. She was started on high dose methylprednisolone and after 3 days of no response she was started on Plasma exchange. Her spastic paraplegia remains unchanged. She has received pressure care, physiotherapy, OT and bowel regimen in the ward. Given her young age, and aggressive disease (developing an severe acute inflammatory myelopathy while on monthly cyclophosphamide pulse therapy), Department of Internal Medicine hopes she can undergo induction therapy with rituximab (375mg/m2) for her seropositive NMOSD in the hopes of avoiding progressive disability and recovering some voluntary function of her limbs.
Laboratory Investigations
CSF Glucose
CSF glucose was 1.4 mmol/L. This is low. It is unfortunately not known what the plasma glucose was at that time, as it wasn’t sent with a plasma glucose sample at the same time, as one would have hoped. If one assumes the plasma glucose have been normal (3.5-5.5mmol/L) and that CSF glucose’s normal range is 0.6-0.8 x plasma glucose, then this value (0.4 – 0.25 that of serum) is significantly low.
Low CSF glucose is indicative of:
- bacterial meningitis,
- mycobacterial infection (TB meningitis),
- mycoplasmal infection and
- fungal infection in the CSF.
- Leucocytes may also decrease CSF glucose – thus it may indicate a disease process rather than only bacterial infection.
CSF Protein
CSF protein of 2.47 g/L (0.15 – 0.45 g/L) is significantly raised. This is indicative of increased permeability of the blood-CSF barrier, most commonly due to inflammatory conditions, but can also be elevated due to:
- Decreased spinal CSF flow above the sampling level due to:
- abscess
- tumor (see also Froin Syndrome)
- collapsed intervertebral disc
- These allow for increased equilibration of fluid between CSF and plasma.
- Immune response within the CSF (intrathecal synthesis of IgG)
- Destruction of brain tissue releasing proteins directly into CSF.
- Neonates (term and pre-term) have a higher reference range – up to 1.7 g/L.
CSF Albumin
CSF albumin of 1271 mg/L (100 – 300) is elevated. This value is increased significantly, likely indicating an increase in the permeability of the blood-brain-barrier (severe impairment).
CSF Albumin Index
The CSF Albumin Index was 31.8 mg/g (<9).
CSF albumin is best interpreted in conjunction with the serum albumin. CSF albumin is corrected for leaking of albumin from the serum (thus incorporating the serum albumin concentration). This is called the CSF albumin index (mg/g) = CSF albumin(mg/L) / serum albumin (g/L)
- <9: intact blood-CSF barrier
- 9-14: slight impairment
- 14-30: moderate impairment
- >30: severe impairment
CSF IgG / Albumin Index
CSF IgG index = 0.86
IgG should under normal situations be almost totally excluded from CSF (blood:CSF ratio of >/= 500:1). Intrathecal production of IgG follows infiltration of the space by B-lymphocytes in demyelinating disorders.
Increase in CSF IgG can however be due to increased permeability form the plasma (dysfunctional barrier), increased plasma IgG concentration or intrathecal production. To correct for the former two, plasma IgG and serum albumin is used in an equation to get the above named index, which tries to isolate CSF IgG for the portion which was produced intrathecally.
The formula is: IgG index= (CSF IgG / Serum IgG) x (Serum Albumin / CSF Albumin). Units of measurement should be similar, at least for serum and CSF respectively.
Reference interval for CSF IgG index is 0.3 – 0.7. Ratios greater than 0.7 indicate increased intrathecal synthesis, as seen in more than 80% of cases of Multiple Sclerosis (MS) and other demyelinating disorders. False elevations occur in traumatic tap and SAH. CSF IgG index is more reliable when the CSF Albumin Index is normal (i.e. when the barrier function is not decreased, but obviously this is rarely the case, as inflammation leads to decreased barrier function).
CSF IgG synthesis rate
153 mg/day
The rate of intrathecal IgG synthesis can be estimated by the empirically derived Tourtellotte’s formula and a synthesis
rate of greater than 8 mg/day is found in most cases of multiple sclerosis. It is a more complex formula, with several constants and probably provides no additional information than the IgG index. (Ref: Tietz 6th Ed.)
Other Investigations
Investigations to this point include the following:
1. MRI brain and spine shows Longitudinal extensive transverse myelitis from the cervical to the lumbar level.
2. FBC and CEU was normal – Neutrophils were normal, lymphocyte count was 0.81.
3. Serologies were ANA, AdsDNA, AntiSm, Anti-Ro Positive. C3 and C4 were normal.
4. HIV, HBV, HCV serology was normal.
5. Serum AQP4 serology positive with a titre of 10
6. CSF: Protein-2.47, Gluc-1.4,P8, L37 R0, IgG index0.87, CLAT, GXP, Culture negative.
7. CD19: 250
8. CXR showed bilateral reticular nodular infiltrate and features of post of TB bronchiectasis
Final Diagnosis
Neuromyelitis Optica Spectrum Disorder
Take Home Message
CSF Glucose
Using a ratio of CSF to serum
glucose ratio of less than 0.4, an 80% sensitivity and 98%
specificity was found for distinguishing bacterial (n = 119)
versus aseptic cases (n = 97) of meningitis.
Donald P, Malan H, van der Walt A. Simultaneous
determination of cerebrospinal fluid glucose and blood
glucose concentrations in the diagnosis of bacterial
meningitis. J Pediatr 1983;103:3. – Referenced from Tietz Textbook of Clinical Chemistry 6th ed.
Recovery from meningitis results in recovery of glucose before CSF cell counts and Total Protein.
CSF glucose is typically normal in CSF viral infections, exceptions may include: Meningoencephalitis with Mumps, EV, HSV, HZV.
Leucocytes may also decrease CSF glucose – thus it may indicate a disease process rather than only bacterial infection.
Ratio of CSF:serum glucose has limited utility in neonates and in pts. with hyperglycemia.
CSF glucose <1.0 mmol/L is highly indicative of bacterial meningitis.
If intellectual disability, seizures and motor impairment is present along with low ratio, think of GLUT-1 transporter deficiency – then measure CSF lactate.
CSF Chemistry
As described above
Correcting total protein for Traumatic tap
The presence of CSF bleeding results in approximately 0.010 g of protein / L per 10^6 RBCs / L
The Vitamin D conundrum
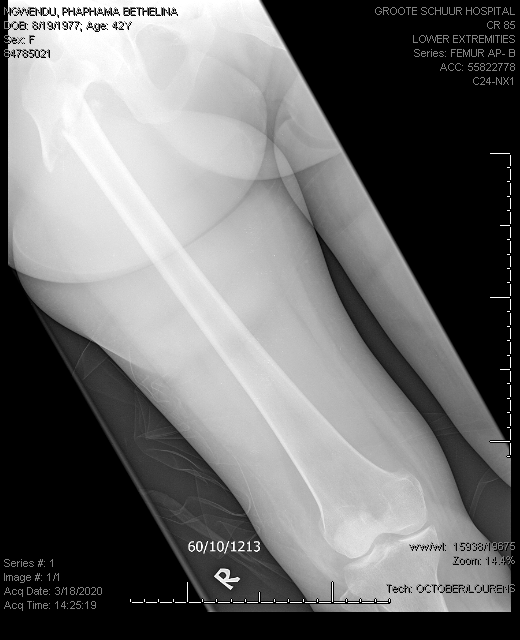
| HOSP # | WARD | F22 Orthopaedics Ward | |
| CONSULTANT | Dr. Jody Rusch | DOB/AGE | 42 Y Female |
Abnormal Result
Total Vitamin D of 27.1 nmol/L on 18 March 2020.
Total Vitamin D of 65.4 nmol/L on 01 April 2020.
Presenting Complaint
Patient had a low impact femur fracture on 18 March 2020 :

History
Patient is known with:
- previous deep venous thrombosis in 2018, on Warfarin therapy
- ?Epilepsy, patient is on carbamazepine, for which the Endocrinology specialists were of opinion that it may have been the cause of the low Vitamin D level.
Examination
Laboratory Investigations
Other Investigations
Final Diagnosis
Vitamin D deficiency likely due to carbamazepine therapy.
Take Home Message
I was not aware that patients on carbamazepine (or other enzyme inducing agents) have lower Vitamin D levels, and it became evident after a quick literature search that it was in fact the case, see the abstract of the article below, also see another article written by a colleague of mine, Jusine Cole, on the Vitamin D controversies.
Also, I have learned that although “total Vitamin D”, as the assay is named in our immunoassay package insert and on TrakCare LIS, has to do with the total portion with regards to protein binding (to Vitamin D binding protein) and not so much to the fact that calcitriol and calcidiol is measured.
It is however evident that, since the cross-reaction in the immuno-assay is quite pronounced with the various forms of Vitamin D, that total indeed, might be an accurate description. In reality, the assay is however called the Total 25-hydroxy Vitamin D.
Vitamin D levels and bone turnover in epilepsy patients taking carbamazepine or oxcarbazepine.
Abstract
PURPOSE:
Evidence suggests that enzyme-inducing antiepileptic drugs (AEDs) may decrease serum 25-hydroxyvitamin D (25-OHD) levels and increase bone turnover. We sought to determine whether these are affected by treatment with carbamazepine (CBZ) or oxcarbazepine (OXC).
METHODS:
We measured serum levels of 25-OHD, parathyroid hormone (PTH), osteocalcin (OCLN), bone alkaline phosphatase (BAP), and urinary N-telopeptides of type I collagen cross-links (NTX) in normal controls (n=24) and in epilepsy patients taking CBZ (n=21) or OXC (n=24) in monotherapy. CBZ patients were subsequently switched overnight to OXC monotherapy, and after 6 weeks, the tests were repeated.
RESULTS:
25-OHD levels were lower in each drug-treated group (OXC, 19.4+/-2.3 pg/ml; CBZ, 20.4+/-2.4) than in the controls (27.5+/-2.8) (ANOVA, p=0.052). This difference was significant for the OXC group (p<0.05). PTH, BAP, and NTX did not differ significantly among groups. OCLN levels were somewhat elevated in the OXC group (2.79+/-0.47 ng/ml) and more clearly and significantly elevated in the CBZ group (3.63+/-0.36) compared with controls (2.38+/- 0.41) (p=0.053). Because the data were very similar between OXC and CBZ groups, they were combined to increase statistical power. The combined drug-treatment group had significantly higher BAP (p=0.02) and lower 25-OHD (p=0.015) than did controls. The latter remained significant even after accounting for the confounding effects of age on 25-OHD levels (p<0.05). No significant differences were found after CBZ patients were switched to OXC.
CONCLUSIONS:
Epilepsy patients taking OXC or CBZ have significantly lower 25-OHD than do normal controls, with a pattern of changes in other bone biomarkers suggestive of secondary hyperparathyroidism. It may be prudent for patients taking CBZ or OXC to be prescribed 25-OHD replacement.
The Vitamin D cutoff conundrum

Introduction
Vitamin D status is considered important for calcium balance and bone health as 1,25 (OH)2 vitamin D (calcitriol) promotes calcium absorption from the gut and has pleiotropic effects in bone. Vitamin D deficiency leads to hypocalcaemia and osteomalacia or rickets in adults and children respectively.
Vitamin D status was also brought under the spotlight owing to an apparent association with cardiovascular health and several other chronic disorders. These associations were noted in animal studies but the findings were not mirrored in humans. Vitamin D sufficiency or insufficiency is determined using quantitative analytical techniques, with results interpreted against statistically-determined cutoffs.
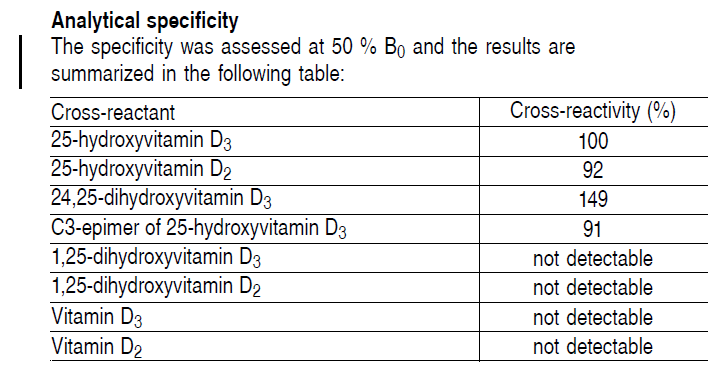
The Controversies
Controversies exist due to the analytical methods as well as the methods to determine these decision limits. The analytical methods available to quantify vitamin D include immunoassays and HPLC or LC-MS/MS methods. The majority of labs use immunoassays to measure 25(OH) vitamin D (calcidiol), and a smaller group also measure calcitriol by immunoassay. Calcidiol occurs at higher concentrations in the serum and, in most cases, it better reflects the vitamin status than calcitriol, as 1-alpha-hydroxylase activity is modulated according to calcitriol and calcium status.
However, immunoassays are non-specific regarding metabolites of vitamin D and therefore results of calcidiol and calcitriol measurement may not be accurate due to cross-reactivity. LC-MS/MS is a much more accurate methodology to measure both calcidiol and calcitriol as well as other metabolites of interest, such as 24,25(OH)2 vitamin D. One controversial point is, therefore, whether or not calcidiol and calcitriol measurements by immunoassay are accurate.
The second controversy lies in the determination of the decision limits for vitamin D repletion, sufficiency and insufficiency. Currently, there are two major sets of decision limits to choose from. The first were determined and recommended by the Endocrine Society based on recommended daily allowances (RDA) for the vitamin. It is argued that the concept of the RDA is misinterpreted and the methods for setting the RDA not understood. These decision limits are high, and by these limits some 50% of most populations are diagnosed with vitamin D insufficiency. This is also dangerous, as replacement of vitamin D may lead to hypervitaminosis D, which is not benign and may in fact increase the risk of falls and fractures. Another consequence is the demand for testing vitamin D levels is very high, which is expensive for healthcare funders or individuals, with questionable health benefits.
The other popular set of decision limits were determined based on the risk of falls and fractures (Institute of Medicine) – a more functional approach. The result of using these limits is that the majority of the population will fall into the vitamin D sufficient or replete groups, and only individuals at high risk will have their status checked and/or monitored and receive supplementation as necessary. This is a more cost- and clinically-effective approach, but is yet to be globally adopted.

The final point to be made is perhaps what drives the interest in vitamin D status, and it may be suggested that it is the reagents and pharmaceutical industry as they stand to gain from increased testing and demand for supplements.
Identification of sample type
| HOSP # | WARD | Red Cross Children’s Hospital, Neurosurgery ward |
|
| CONSULTANT | George van der Watt | DOB/AGE | 11y Male |
Abnormal Result
CSF Glucose: <0.1 mmol/L
CSF Protein: <0.01 mmol/L
Both of the above results have already been rerun on the same analyzer with the same result.
Presenting Complaint
It was then suspected in the lab that the results might have been obtained from a urine (or other fluid) sample rather, which might accidentally been registered / recorded as CSF.
An MC&S (Microscopy, Culture and Sensitivity testing) was also requested on an aliquot of the sample.
History
The above result was obtained from a patient known with hydrocephalus. No other information was available at the time of analysis.
Examination
N/A
Laboratory Investigations
As above abnormal results.
Other Investigations
Microscopy: No leucocytes; No bacteria; India Ink stain was pending.
The following possibilities were thought of:
- Pre-analytical factors:
- A urine sample was sent and incorrectly registered as CSF
- A possibility to quickly exclude this was to determine the creatinine on the sample if urine, then the creatinine will measure in the thousands (umol/L) or in the mmol/L range.
- One could also do CSF identification by CSF electrophoresis for the presence of beta-2 transferrin or beta trace protein identification, but this is expensive and laborious.
- Bacteria metabolised all the glucose, and for some reason the protein did not go up in the patient, although the protein <0.01g/L is extremely low, making the possibility of this scenario unlikely.
- A urine sample was sent and incorrectly registered as CSF
- Analytical factors:
- Bubble aspiration, although the rerun gave a similar result.
- Interferents: none could be thought of in this scenario.
- Post-analytical:
- The result was obtained directly from the analyzer’s user interface, hence making transcription / translation errors unlikely.
Final Diagnosis
The clinician, a neurosurgery doctor, was phoned to enquire about the history, and it was indeed a sample from the cerebro-spinal space, but upon questioning the Neurosurgery doctor, it became known that:
- This sample was obtained intra-operatively during placement of a ventriculo-abdominal shunt for hydrocephalus
- During the procedure, the ventricles have been flushed with Normal Saline, which explains the low CSF protein and the low Glucose.
Take Home Messages
The history from the clinician was confirmation that this sample was indeed from the cerebrospinal space, although not representative of the cerebrospinal space, as it was taken during a procedure, hence likely pure saline was measured.
Adequate history from the clinician is most often the most useful information that can be obtained, especially when severely abnormal results are obtained.
When results do not make sense, one should not authorize them without discussing with the clinician first.
The neurosurgery doctor agreed that to request the chemistry on this sample was not indicated and they actually only wanted the Microbiology investigations as proof of some sort that an infection was not present, for which exact indication the Microbiology team might comment on.
Results was thus not authorized, but rather cancelled with a comment, stating that sampling was not representative of the physiological CSF.
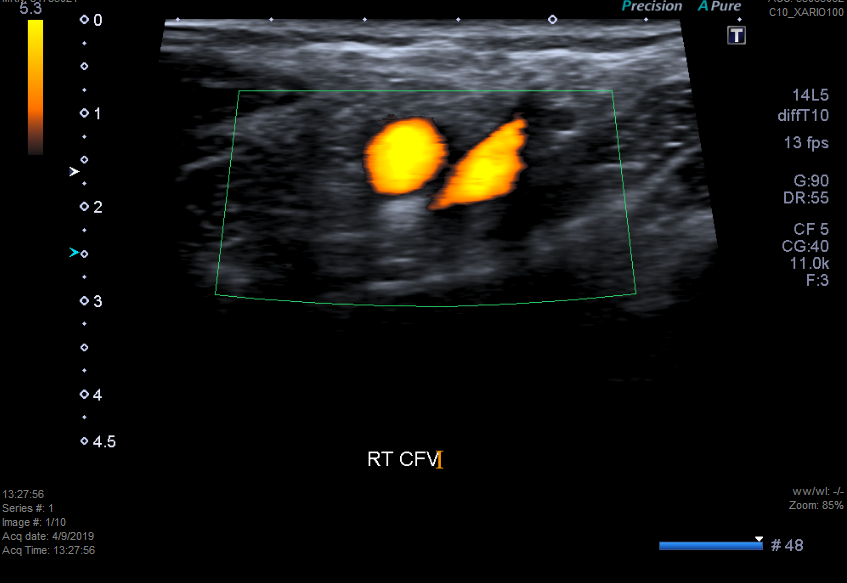
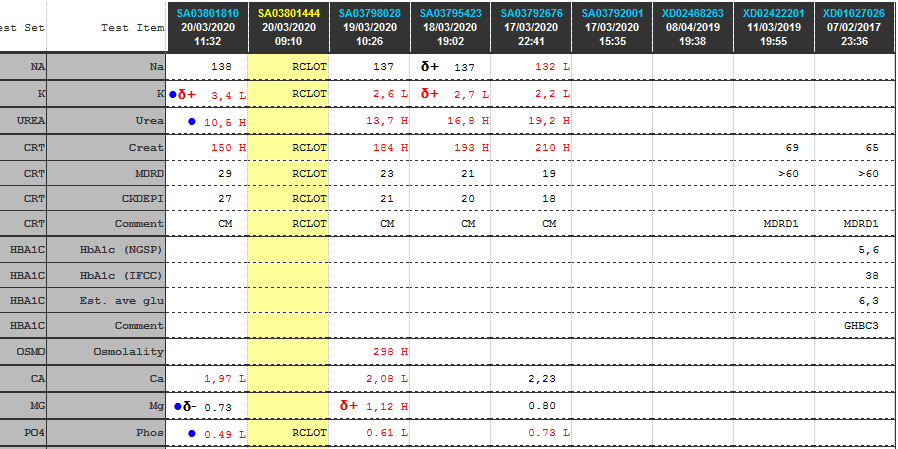
A case of renal tubular potassium loss
| HOSP # | WARD | Internal Medicine Ward | |
| CONSULTANT | Heleen Vreede | DOB/AGE | 86 year old lady |
Abnormal Result
Hypokalemia in a 86 year old lady.
Presenting Complaint
Muscle weakness for the preceding 3 weeks.
History
Known with hypertension, dyslipidaemia and chronic kidney disease.
Presented at a private practice with symptomatic hypokalemia. Patient gave a history of 3 weeks body weakness and dizziness and said she hasn’t been eating well for the prior three weeks.
No other symptoms. No previous medical admissions or procedures.
The patient has just had persistent hypokalemia in hospital despite supplementation. The consultant in Internal Medicine attributed her persistent CMP disturbances to refeeding type syndrome.
In the hospital admission the patient was receiving:
- Simvastatin 20mg dly PO
- Calcium carbonate (1g elemental Calcium) q8h PO
- SlowMag 2 tabs daily PO
- Metoclopramide 10mg q8h PO
Examination
Not available
Laboratory Investigations
Other Investigations
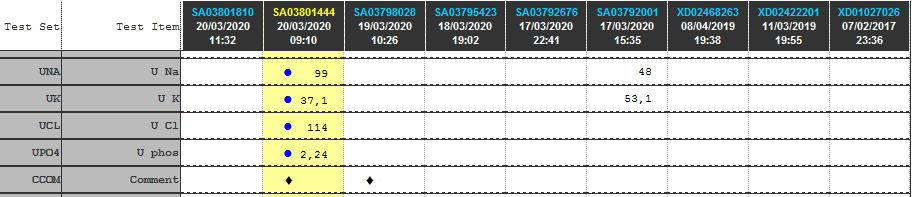
Transtubular Potassium Gradient (TTKG)
TTKG (Transtubular potassium gradient)………… 8.16
TTKG values between 8 and 9 are considered normal in patients with a normal diet.
TTKG >/= 3 in hypokalemia suggests renal potassium wasting.
Ref: Ethier JH et al. Am J Kidney Dis. 1990 Apr;15(4):309-15. The transtubular potassium concentration in patients with hypokalemia and hyperkalemia.
Values used for calculation:
Urine K…………… 37.1 mmol/L
Serum K……………. 3.4 mmol/L
Urinary Osmol ……… 396 milliosmoles
Plasma Osmol ………. 296 milliosmoles
Fractional Excretion of Potassium (FEK)
FEK ……………………………………. 45 %
Tubular reabsorbtion of potassium (1-FEK)….. 55 %
Values used for calculation:
Urine K…………….. 37.1 mmol/L
Serum K……………… 3.4 mmol/L
Urine Creatinine …….. 3.6 mmol/l
Serum Creatinine …….. 150 umol/l
Final Diagnosis
Take Home Message
A study by Elisaf, M & Siamopoulos, KC (Postgrad Med J 1995; 71: 211-212), clearly showed that in patients with hypokalaemia of extrarenal origin FEK is less than 6.5%, i.e. a FEK more than 6.5% is indicative of inappropriate potassium loss. FEK was more than 9% in all patients with hypokalaemia of renal origin.
The study concluded that in hypokalaemic patients with normal renal function, FEK is a useful tool in the diagnostic approach of hypokalaemia.
Limitations: A random urine sample was used to determine these values. Ideally a 24 hour urine collection should be used and theoretically should provide a more accurate estimation of tubular function. The fractional excretion of potassium is however inherently normalized to creatinine.
No clinical info / medication history was supplied. The most likely cause of inappropriate potassium loss in the urine is medication (iatrogenic) like diuretics and some antihypertensives. Ideally, if a pathogenic, rather than iatrogenic cause of potassium loss is suspected, the patient needs to be free of potassium supplementation and all medication which could influence tubular function must be stopped before analysis of the renal tubular electrolyte handling.
Absorbance values >2, theoretically possible?
I’ve been boggled by this question in the topic ever since I
got absorbance readings on an ELISA test kit >2, up to Absorbance units of
3.5 and so on.
I speculated how it could be possible, and with George’s
explanation came up with all sorts of theories that plate readers probably
correct for the light path etc.
In my mind, since the formula for absorbance is the following: Abs = 2 – log (%T), my thoughts were that it is impossible to have absorbance values more than 2. Hence I thought Abs. should be discarded above 2.
I have however seen on this page,
which explained it quite well with a table, that it is indeed possible to
obtain absorbance values >2 if the light source is strong enough and the
spectrophotometer is sensitive enough to obtain accurate readings in this
range.
The theory is however, when the transmittance of <1% happens, log part of the formula (log%T), becomes a negative value. One thus subtracts a minus, theoretically making absorbances possible to indefinite values.
| Absorbance (optical density) |
Transmittance % |
| 0 | 100 |
| 1 | 10 |
| 2 | 1 |
| 3 | 0.1 |
| 4 | 0.01 |
| 5 | 0.001 |
| 6 | 0.0001 |
“At an absorbance of 6, only one 10,000th of one percent of a particular wavelength is being transmitted through the filter (lens). Absorbance is measured with a spectrophotometer, which establishes the light transmission and calculates the absorbance. However, the spectrophotometer can only measure absorbance up to 4.5 directly. Beyond this level all values must be extrapolated. For example, if a 2 mm thick filter is measured to have an absorbance of 3, then it is assumed that a 4 mm thick filter should have an absorbance of 6.”
Obviously there are still limitations to this and the general principle remains that absorbance units should be sought to be <1.8 (actually ideally now that I think of it <1.0) to make the standards and measurements more in the linear range (i.e. %Transmittance less than (100-10^10)=<90), for Abs. <1. I do think however that spectrophotometers (and plate readers in particular) these days are probably more sensitive than historically and hence one could go up a bit with the absorbance, given the understanding of the limitations regarding imprecision at these Absorbance levels.
One should understand that the absorbance >2 units does measure light intensity at a %Transmittance value between 99% and 100%, hence the room for error becomes exponentially bigger if the spectrophotometer’s CV is not precise enough at these %T values.
Still to be revealed to me is the fact that absorbance
values I obtained in Spectrophotometers and plate readers often did not
correlate well, even when correcting for the light path length, and I would
probably just need to read more to get proper clarity, or the path length
through the well in the plate reader was not accurately measured by me.
One way to correct for path length of water could be to measure the absorbance
of the water / solvent at 977nm (infrared; IR) and correct therefor, but most
specs we use don’t have IR measuring capabilities.
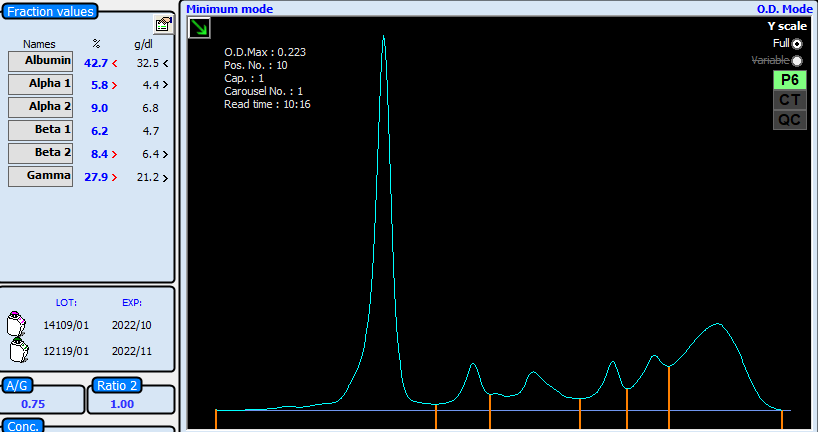
Query High Dose Hook effect on Estradiol
| HOSP # | WARD | Andrology Clinic (IVF Clinic) | |
| CONSULTANT | Heleen Vreede | DOB/AGE | 35 y Female |
Abnormal Result
Estrogen 4823 pmol/L in a patient with in vitro vertillization.
Presenting Complaint
The Doctor called, querying if this might be a possible high dose hook effect. They expected a much higher result with this particular patient.
I explained that this is a competitive immunoassay and that high dose hook effect is most likely observed rather with sandwich immunoassays.
History
This patient was undergoing IVF for multiple pregnancy – higher value anticipated (10000 – 12000 pmol/L)
Examination
N/A
Laboratory Investigations
1 in 10 dilution made, result of the rerun was 415 x 10 = 4150 pmol/L (-14% difference).
Other Investigations
Final Diagnosis
The estradiol was indeed likely close to a true result, even though queried by the clinician.
This was confirmed by the duplicate result when running this sample in dilution. The -14% difference from the original result can likely be explained by imprecision from:
- Pipetting error when doing the manual dilution
- Imprecision of the analyser
- Matrix effects when using the universal diluent from the analyser
Take Home Messages
Competitive immunoassays are NOT prone to high dose hook effect, due to the inherent characteristics of the assay.
It is however known that measurement of estradiol at the levels required for IVF is not in the linear range of the assay and that there are likely to be imprecision as noted by the points above.
The measuring range as quoted by the package insert for our Roche Cobas 6000 E2 assay is 18.4 – 11010 pmol/L (LOD to max of master curve). It can however be reported up to 110100 pmol/L for 10-fold diluted samples.
It is however a pity that the reading off the standard curve (signal) cannot be seen on the analyzer’s firmware, as can be seen with routine chemistry analytes eg. liver enzymes etc.
An interesting article which I’ve also forwarded to the doctor is added below.
PDF Loading...
A falsely normal OGTT result?
| HOSP # | WARD | Vanguard Antenatal Clinic | |
| CONSULTANT | Jody Rusch | DOB/AGE | 32 y Female |
Abnormal Result
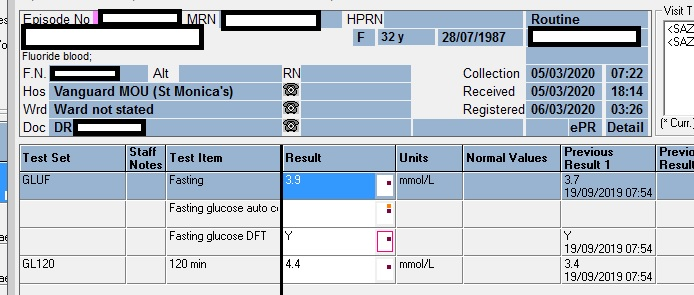
Oral glucose tolerance test with the Sodium Fluoride (NaF) tubes registered by the lab 20 hours after being sampled.
Collection date: 07h22 05/03/2020
Received date: 18h44, 05/03/2020
Registered date: 03h26, 06/03/2020
Please note that samples in our lab are being centrifuged after being registered.
| Fasting Glucose | 3.9 | mmol/L |
| 120 min. Glucose | 4.4 | mmol/L |
Presenting Complaint
My thoughts were, that if the sample isn’t centrifuged in a timely manner, metabolism would still happen, albeit at a slower rate. I also thought that metabolism (glycolysis) would continue if left for a long period (>8 hours) uncentrifuged.
Would you argue the result as given below at “Laboratory Investigations” is reliable, given the following info?
- Stability of glucose in whole blood in NaF tubes?
- Could this be a false normal result?
The stability spreadsheet as summarized by our lab did not have the stability info for glucose in whole blood:

History
Patient is most likely pregnant (being from an antenatal clinic) and this is then a screening test for gestational diabetes.
Examination
N/A
Laboratory Investigations
Other Investigations
Literature search on Google Scholar yielded the following interesting article:
Effectiveness of sodium fluoride as a preservative of glucose in blood.
A Y Chan, R Swaminathan, C S CockramClinical Chemistry, Volume 35, Issue 2, 1 February 1989, Pages 315–317, https://doi.org/10.1093/clinchem/35.2.315 Published: 01 February 1989
Abstract
How effective is sodium fluoride as a preservative of blood glucose? We compared changes in glucose concentration in fluoride-treated blood specimens with those of heparin-treated specimens. The former declined rapidly during the first hour; thereafter the rate of decrease was slower, and after 4 h the glucose concentration in the blood samples remained stable for up to three days. In contrast, the glucose concentration in the heparin-containing samples declined continuously. During the first hour, however, the rates of decline in the two types of samples were similar. Evidently sodium fluoride takes effect slowly but effectively in preserving glucose in blood for at least three days. Its use, however, is unnecessary if the concentration of glucose is to be measured within the first hour after sampling.
Final Diagnosis
This is likely a true result, meaning the patient is normal and does not have impaired glucose tolerance, nor diabetes.
Take Home Message
Blood glucose is stable for 3 days in plasma from NaF tubes, whether being centrifuged in a timely manner or not.
The stability of glucose in specimens is affected by storage temperature, bacterial contamination, and glycolysis. Plasma or serum samples without preservative (NaF) should be separated from cells or clot within half an hour of being drawn. When blood is permitted to clot and to stand uncentrifuged at room temperature, the average decrease in serum glucose is ~7% per hour (0.28 – 0.56 mmol/L/hour), as a result of glycolysis. Glycolysis can be inhibited by collecting the specimen influoride tubes (1).
(1) Sacks DB. Carbohydrates. In: Tietz NW, ed. Fundamentals of Clincal Chemistry. 4th ed. Philadephia: WB Saunders 1996;351-374.
A case of low urine creatinine
| HOSP # | WARD | Sample from porphyria laboratory | |
| CONSULTANT | Dr. Heleen Vreede | DOB/AGE | 29y Female |
Abnormal Result
Presenting Complaint
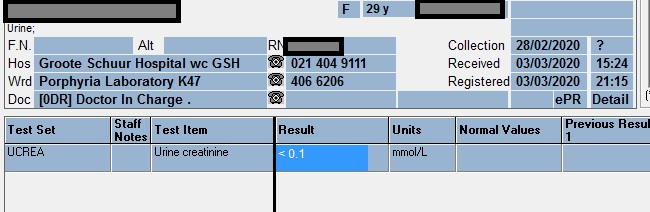
Upon signing blood results out, a creatinine result was measured by the analyzer as <0.1 mmol/L on a urine sample.
History
Clinical History was not available, but in my personal experience at the time, I haven’t seen such a low urine creatinine yet.
The possibilities in my mind, was that this was either a serum sample and could perhaps be incorrectly sent / registered from the Porphyria lab as serum, hence the result being < 0.1 mmol/L (<100umol/L if translated into serum reporting units).
Examination
The sample smelt and looked like urine. According to our new registrar, Mrs. Mariam Mahomed, it also tasted like urine. I was personally not capable of this task, so we decided to rerun the sample.
Mrs. Bilqees Jacobs, our technologist on the bench this day was of opinion that when such a low result is seen, it is usually due to a bubble aspirated by the analyzer’s sampling probe.
Laboratory Investigations
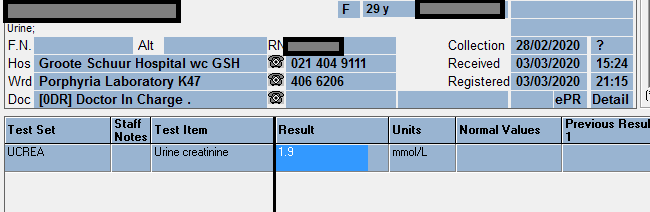
The rerun of the sample as a urine creatinine gave the result as 1.9 mmol/L, more in keeping with a true urine creatinine result.
Other Investigations
None was necessary, but should the result have been < 0.1 mmol/L on the rerun, we would then have run the sample as a serum on the analyzer to more accurately quantify the value.
Final Diagnosis
Possibly, a bubble was aspirated by the analyzer’s sampling probe and hence it did not pipette enough sample into the reagent well, or likely not pipette any sample therein.
Take Home Messages
Try to avoid bubbles in samples.
This brings me to the point: whenever a ” lower than detection limit” is seen, think of the cause:
“Tiny Bubbles!”
Hypocalcemia with Hypomagnesemia
| HOSP # | WARD | Internal Medicine ward | |
| CONSULTANT | George vd Watt / Heleen Vreede / David Marais | DOB/AGE | 58 y Male |
Abnormal Result
Upon signing out blood results:
Calcium = 1.41 mmol/L – Critically low Calcium result
Magnesium = 0.37 mmol/L – Critically low Magnesium
Presenting Complaint
Loss of breath initially accompanied by weight loss.
Upon admission to the ward, patient was slightly delirious, but still able to walk and talk.
History
Patient with metastatic lung cancer and accompanying hypercalcemia, a week prior to the results as at present.
Doctor has given IV Bisphosphonate after the hypercalcemia was noted a week prior (Calcium = 4.23 mmol/L; Alb = 21 g/L; Corrected Ca = 4.61 mmol/L)
Examination
Extensive Crepitations over all the right lung fields.
Laboratory Investigations
Other Investigations
Final Diagnosis
Invasive lung CA with “hungry bones” after IV Zolendronic Acid
Vitamin D deficiency, preventing Calcium absorbtion after the Zolendronic acid started its action of inhibiting bone resorption.
Take Home Messages
CA causes hypercalcemia
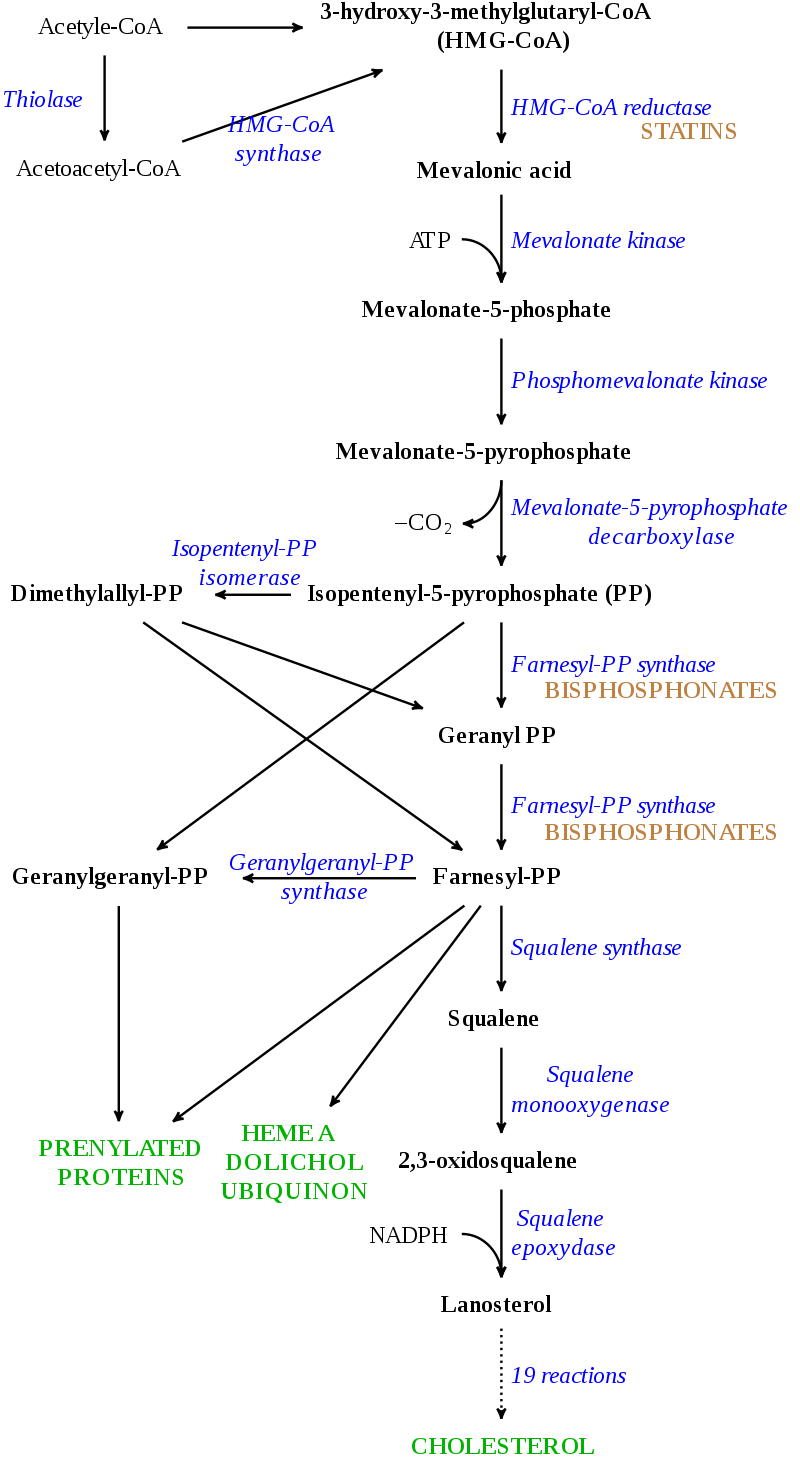
Bisphosphonates inhibits bone resorption. Because 99.95% of Ca in the body resides in bone, the effect in serum (the remaining 0.05% of total body Ca) can be significant.
All bisphosphonate drugs share a common phosphorus-carbon-phosphorus “backbone”:

They differ in the R-groups as above. It binds to calcium hydroxyapatite in bone.
Of the dose infused / absorbed, 50% is excreted unchanged by the kidney, the rest binds to bone tissue, where its elimination half life can apparently be up to 10 years! (UW Courses Web Server- https://courses.washington.edu/bonephys/opbis.html )
Because a bisphosphonate group mimics the structure of pyrophosphate, it can inhibit activation of enzymes that utilize pyrophosphate.
Magnesium follows Calcium levels, but Mg deficiency itself can also cause hypocalcemia.
Wilson’s disease
Mutation in the Wilson disease protein (ATP7B) gene, a protein transporting excess copper to bile.
Copper build-up in the brain and liver mostly, which can cause fulminant liver failure.
Other organs
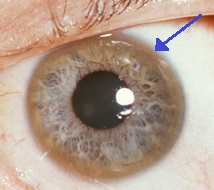
Eyes: Kayser-Fleischer rings
Kidney: RTA type 2
Heart: Cardiomyopathy
Hormones: Hypoparathyroidism
Diagnosis
- Serum and urine copper:
Urine copper Interpretation:
Normal dU copper (24 hr) ………………… 15-36 ug/24hr
Indicative of Wilson’s Disease …………… 40-100 ug/24hr
(Need to confirm with additional test)
Confirms Wilson’s Disease ……………….. >100 ug/24hr
Serum Copper will paradoxically be low. This is because ceruloplasmin (copper-binding protein) is low in 80-95% of patients with Wilson’s disease.
2. Ceruloplasmin low (remember it’s an acute phase protein)
3. Liver biopsy
4. Genetic sequencing of the ATP7B gene.
Treatment
Low Copper diet (avoid copper cutlery)
Penicillamine (Cuprimine – not available in South Africa) binds Cu by chelation and excretion in urine (but causes drug-induced lupus and Myastenia Gravis in 20%)
Trientine also chelates.
Zinc stimulates metallothionein, a protein in gut cells that binds copper and prevents their absorption and transport to the liver. As soon as urine Cu excretion is in normal limits, patients will go on to Zn therapy.
Asymptomatic pts. (by family gene screens) are treated, because copper accumulation will cause problems later. Usually Zn is used.
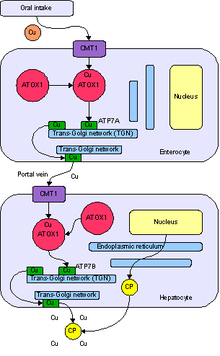
Images are all from Wikipedia

Acute poisoning causing few to “fall flou”
| HOSP # | WARD | Casualties | |
| CONSULTANT | George van der Watt | DOB/AGE | 26 & 50 y/o males |
Abnormal Result
Urine toxicology screening / Urine organic acid analysis
Presenting Complaint
ESKOM load shedding resulted in failure of the power supply (including the emergency power generator) at a part of the hospital which included the routine toxicology screening lab at the Department of Pharmacology.
Two patient samples arrived at Red Cross Hospital IMD lab one Wednesday morning, brought personally by the Lab Manager of the Pharmacology Toxicology Department, requesting help to identify the cause of poisoning in two of six patients with alleged poisoning. At the time, the patients were both on ventilatory support in ICU due to depressed level of consciousness.
The repeated electricity power failures over a weekend, resulted in Toxicology’s state-of-the art tripple-quad tandem qTOF mass spectrometer to fail.
History
Six individuals were given a drink by a taxi driver in Landsdowne, Cape Town, on that Monday morning, all who collapsed few minutes later in the streets. Paramedics were on the scene soon and all affected patients were rushed to respective hospitals. See more on the Daily Voice.
Examination
The two individuals from whom we obtained urine for analysis, both had similar signs:
GCS was apparently 4/15, requiring intubation and ventilation.
Pupils were not miotic nor midriatic and signs were not in keeping with organophosphate poisoning.
Laboratory Investigations
No other laboratory investigations were available at the time. In retrospect, one of the patient’s results are available and serum electrolytes, liver enzymes, liver function and renal function tests were within normal range.
Other Investigations
Urine organic acid analysis by GC-MS were done by us that day and we could identify Gamma-hydroxybutyrate (GHB) with an accurate hit to a known library adequately. We also ran a control urine sample of myself to prove the absence thereof as a negative control.
In the chromatograms below, note the height of the base peak, Pentadecanoic Acid (PDA) in relation to the peaks eluting at 11.45 minutes, 4-OH-butyrate, the analyte of interest. It can be seen that it is present in both the patient’s samples and is absent in the control sample.
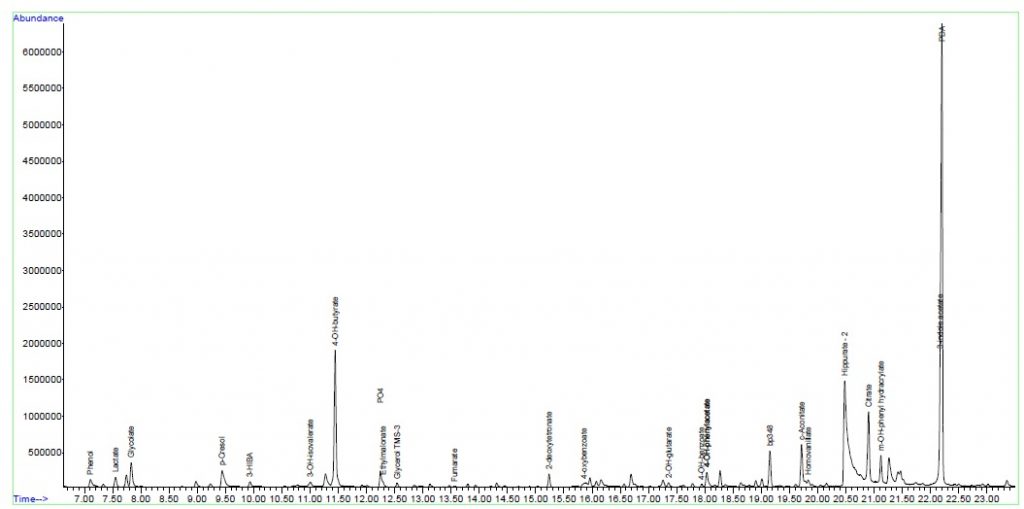
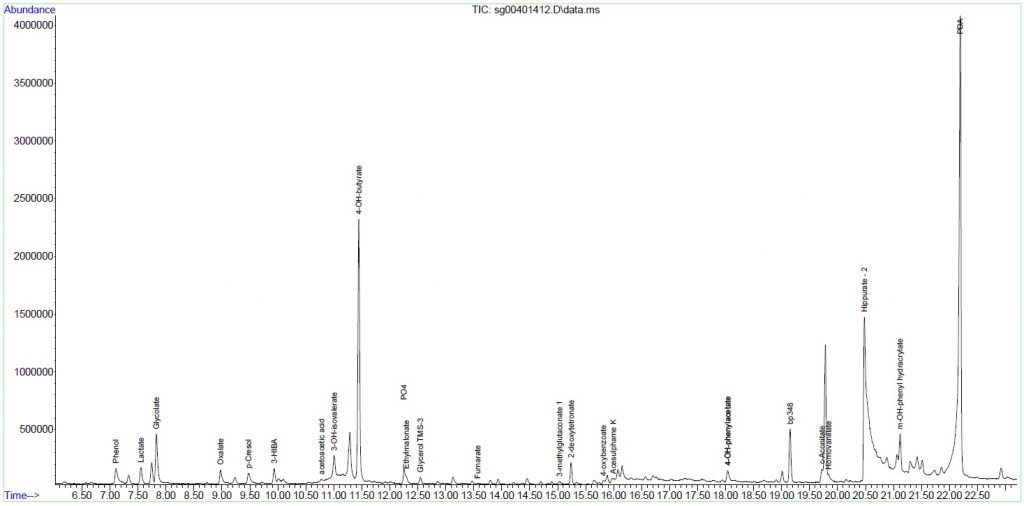
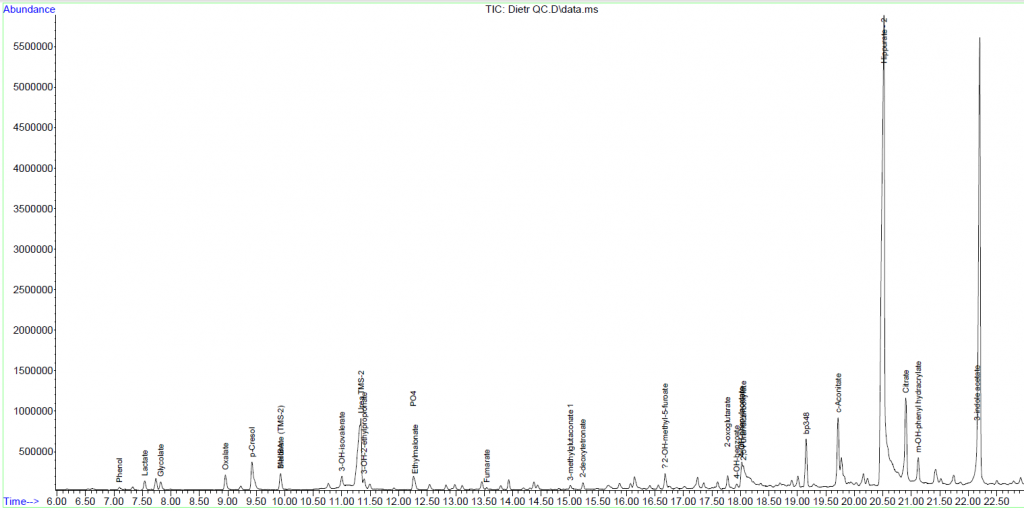
Final Diagnosis
It was confirmed that both cases as analysed by us was in keeping with intoxication with 4-OH-butyrate (gammahydroxybutyrate; GHB).
Take Home Messages
We concluded that cases of gammahydroxybutyrate intoxication can be confirmed by urine GC-MS analysis at our IMD chemistry lab at Red Cross Children’s Hospital.
Gammahydroxybutyrate (GHB) has appeared to be quite a common (and perhaps re-emerging) drug in the Cape Town area. It can relatively easily be manufactured without sophisticated equipment and due to its ease of manufacture is not extensively made / traded by illicit drug traders.
GHB (an agonist of certain GABA receptors) can be manufactured relatively easily by addition of two ingredients, a prodrug gammabutyrolactone (GBL; a commercially available product) and an alkali hydroxide, such as sodium hydroxide to form GHB salt.
Other trade names of GHB include “Liquid Ecstasy”, “lollipops”, “Liquid X” or “Liquid E”.
See below a copy of the article as it appeared in the Daily Voice, a Cape Tonian newspaper:

A case of hyperuricemia in the ICU
| HOSP # | WARD | Surgical ICU | |
| CONSULTANT | Heleen Vreede / George van der Watt | DOB/AGE | 30 year Male |
Abnormal Result
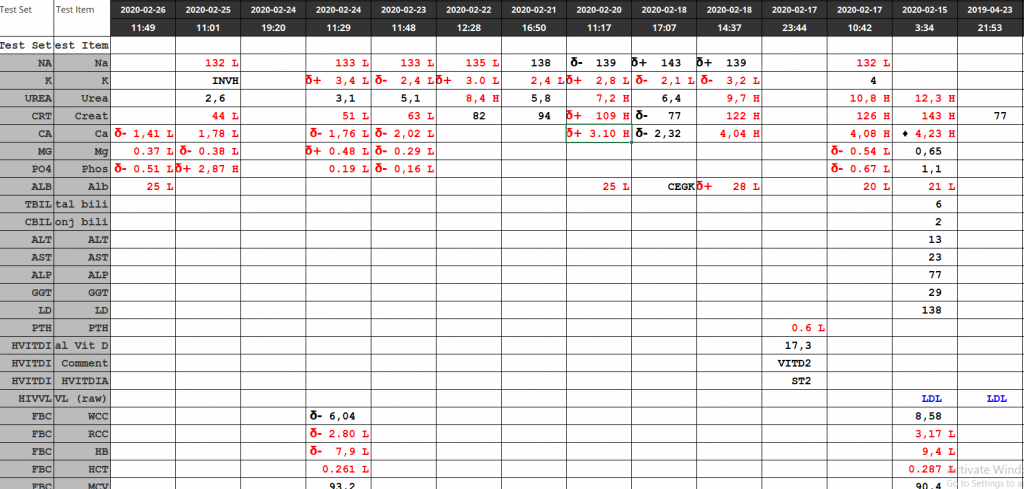
The result upon the query being raised by the reviewer was a uric acid of 0.95 mmol/L (0.21-0.43 mmol/L). Three days prior to this result, the patient had a uric acid serum concentration of 0.38 mmol/L.
Presenting Complaint
The patient presented to the hospital with a history of a swollen tonsil unilaterally. This worsened over few days to a severe infection (sepsis) as described below.
History
No significant history. Patient reported sober habits.
Examination
At initial presentation, the patient appeared to have a suppurative tonsillitis. The tonsillitis later developed into a retropharyngeal abscess and soon extended into the thorax, forming a pericardial abscess, which is what was found clinically at the time of admission to Groote Schuur Hospital.
Laboratory Investigations
Date: newest to oldest (only chemistry results included)

Other Investigations
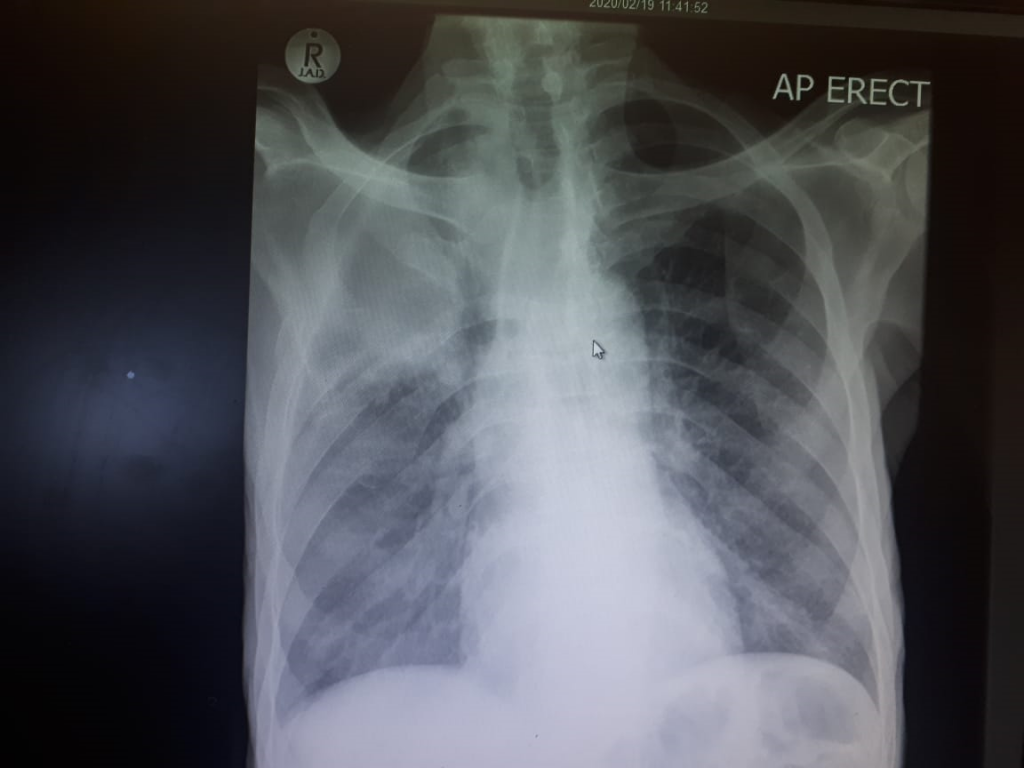
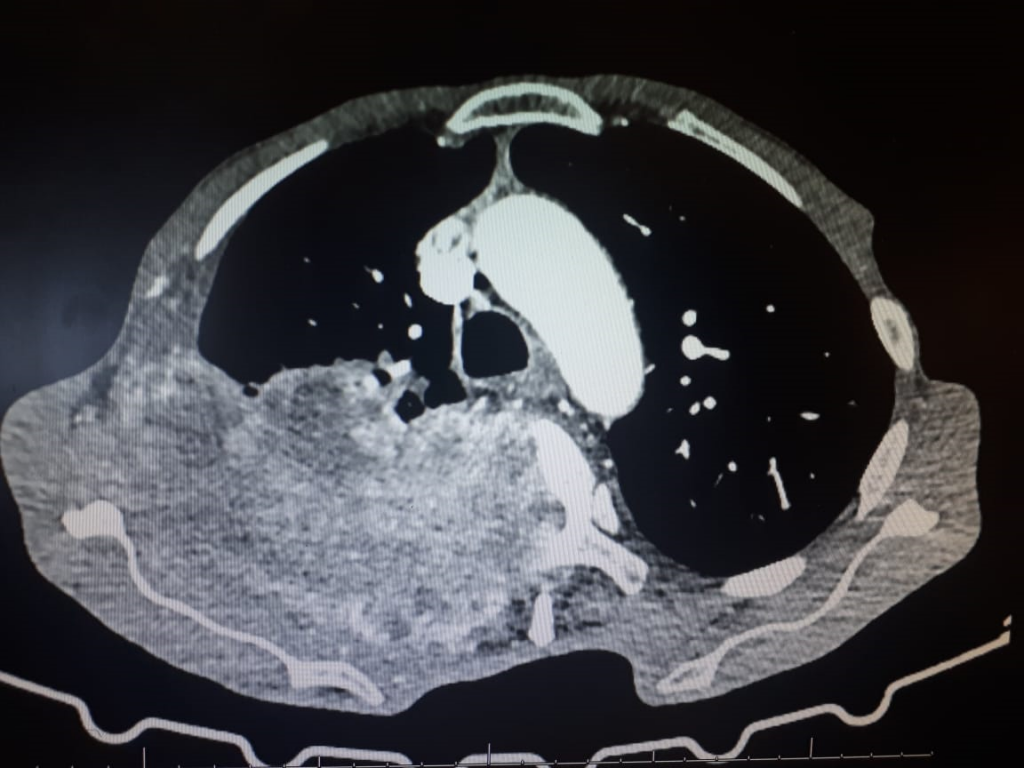
CT scan: images to follow
Final Diagnosis
Retropharyngeal abscess progressing to a thoracic abscess and causing overt signs and symptons of heart failure.
Patient required a thoracotomy and pericardial drainage of the abscess.
Take Home Messages
- Do not take tonsillitis lightly. If not adequately managed, it may cause serious complications.
- Elevated Uric acid is a risk factor for acute kidney injury. This may be by means of acute gouty crystal deposition, but other crystal-independent roles has also been described.
- Uric acid concentration will rise significantly in severe infection, most likely due to the fast tempo of tissue or DNA turnover, both by bacteria and host tissue breakdown and repair. Uric acid is a product of the metabolic breakdown of purine nucleotides.
- Uric acid, being a heterocyclic compound, I thought could interfere in various assays, and I thought even in the Jaffe reaction for creatinine, but it doesn’t seem to be a common interferent when doing a quick literature search.
- Uric acid appears to be the major anti-oxidant in human serum constituting around 61% of total anti-oxidant activity, evidenced by Maxwell et al.:

- Relative contribution to total serum anti-oxidant activity in this study was: urate 65.1%, vitamin C 8.7%, vitamin E 10.6%, vitamin A 5.7%, thiols 7.8% (as in albumin) and bilirubin 1.9%.
- One immediately thinks that a patient with such a rapidly progressing infection has to be immunocompromised, the most common cause(s) in South Africa being HIV or diabetes mellitus. This patient however was HIV negative, according to HIV ELISA and did not have reported signs and symptoms of diabetes.
PTH Summary
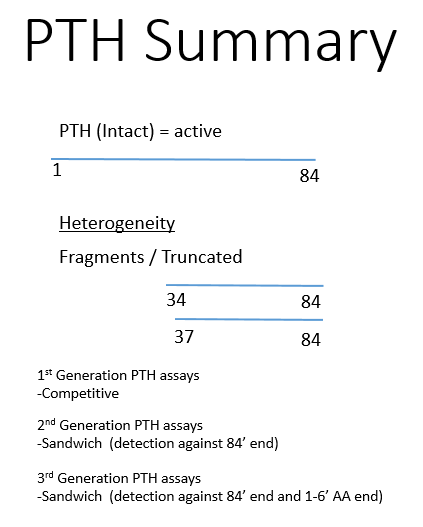
n-truncated are deficient in the first few aa’s (7-84) – hence biologically inactive.
1-11 aa sequence is necessary for function.
Different assays:
- Intact PTH measurements: 7-84 and 1-84
- Bioactive PTH: 1-84
- CAP assay: cAMP inducible PTH. This assay determines the biologically active PTH by its ability to induce cAMP.
- PTHrP assays and PTH assays are exclusive to each other by design.
A Case of Neurodevelopmental Delay
| HOSP # | WARD | Neurodevelopmental clinic – Inkosi Albert Luthuli Hospital | |
| CONSULTANT | Prof. George van der Watt | DOB/AGE | 2y male |
Abnormal Result
Urine organic acid analysis was performed upon which a big peak was seen, representative of phenylpyruvate.
Presenting Complaint
The patient was a 2 year old male evaluated at a neurology clinic for neurodevelopmental delay.
History
The patient’s brother died at 3 or 4 years of age with similar neurodevelopmental delay.
Examination
Unfortunately this information was unavailable. The clinician I got hold of at Inkosi Albert Luthuli hasn’t seen the patient himself.
Laboratory Investigations

Other Investigations
The urine amino acid analysis yielded a significantly raised phenylalanine: 672 umol/L (ref <67)
Final Diagnosis
This is a case of phenylketonuria
The diagnosis is also supported by a plasma phenylalanine of 672 umol/L (ref < 67).
Take Home Messages
Build-up of phenylalanine gets metabolised to phenylpyruvate (which is seen in urine at high levels).
Phenylalanine levels >600 umol/L in serum is highly indicative of phenylketonuria
Prof. George van der Watt
Biopterin cycling defects usually cause levels >125 umol/L.
This deficiency is 4-monooxygenase deficiency.
Management of PKU is with a phenylalanine restricted diet.