Mr. X, a 66 year old male, complained of chest pain, was seen at the Oudtshoorn Emergency department and a myocardial infarction was excluded by three serial point-of-care (POC) Troponin I results.
History
Known with hypothyroidism, but the cause was not defined yet.
On Eltroxin 150 ug daily PO
No other treatment.
Various stool analyses had been sent in for culture, with no definitive result.
Examination
Unfortunately not known.
Laboratory Investigations
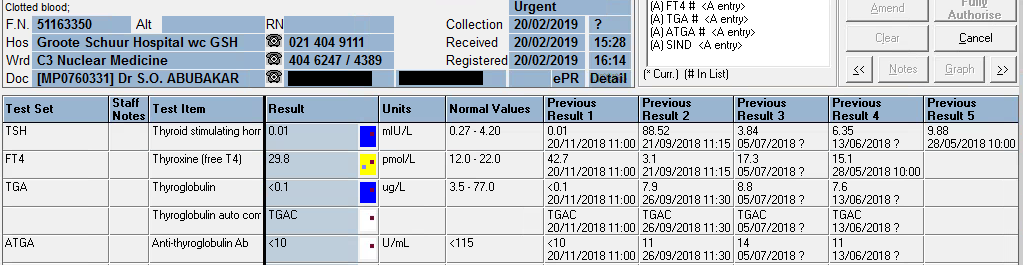
Free T4: 24.6 pmol/L (7.6 – 16.1 pmol/L)
Anti-Thyroglobulin Antibody levels were elevated at 1944 U/mL (ref. <115 U/mL).
Other Investigations
Later, by retrospective viewing of the patient’s results it was revealed:
Total Cholesterol (TC) was elevated at 7.6 mmol/L. Hypothyroidism is associated with hypercholesterolemia. It can be concluded by the retrospective overview of results that upon an episode of hypothyroidism, the patient had hypercholesterolemia. This was most likely due to cessation of Thyroxine treatment, to whatever reason.
Index sample marked by the yellow shade. TC result which is raised (upper left corner) corresponds to the severely hypothyroid episode as revealed by the low T4 on that same sample.
Investigations also confirmatory for auto-immune hypothyroidism are:
Anti-Thyroid peroxidase antibodies
Anti-TSH receptor antibodies
Final Diagnosis
Auto-immune hypothyroidism
Take Home Messages
Interestingly, numerous patients with hypothyroidism is diagnosed at our Lipid Clinic at Groote Schuur Hospital. Patients are being referred for hypercholesterolaemia. Generally referral to this clinic happens when TC > 7.5 mmol/L. These patients are referred as presumed to have familial hypercholesterolaemia, but upon further work-up it is found that many of these patients have long-standing untreated hypothyroidism.
Prevalences of antithyroid antibodies as summarized by Up-to-date:
Thyroglobulin value of <0.1 ug/L upon signing results out.
Presenting Complaint
Patient presented with a neck “swelling” in October 2016. Systemic complaints were not inquired, but none was reported.
History
TFT: euthyroid since presentation when the thyroid functions were first tested in 2016.
Examination
A solitary thyroid nodule was found in the neck, moving with swallowing.
Laboratory Investigations
TFT: euthyroid upon presentation, which is clear from the table below.
07/11/2019
08/08/2019
21/06/2019
20/02/2019
20/11/2018
26/09/2018
21/09/2018
05/07/2018
13/06/2018
29/05/2018
07/05/2018
08/01/2018
05/04/2017
26/10/2016
TSH
δ- 1,49
δ- 7,07 H
δ+62,97 H
0.01 L
δ- 0.01 L
δ+88,52 H
3,84
6,35 H
δ+ 9,88 H
2,86
4,05
δ+ 3,26
1,62
Free T4
21,4
δ+ 22,3 H
δ- 3.0 L
δ- 29,8 H
δ+ 42,7 H
δ- 3,1 L
17,3
CEGK
15,1
δ+ 14,9
12
Free T3
4,8
Thyroglobulin (3.5-77.0 ug/L)
<0.1 L
<0.1 L
0.1 L
<0.1 L
δ- <0.1 L
7,9
8,8
7,6
Anti-thyroglobulin Ab (<115 U/ml)
<10
<10
<10
<10
<10
11
14
11
From results above it can be seen that the patient was euthyroid upon presentation (in 2016 and later until excision – highlighted in bold)
Hemithyroidectomy was done in May 2018, and another hemithyroidectomy in September 2018, thus the thyroglobulin after the first and second surgery was still detectable, but absent after September 2018.
Other Investigations
Ultrasound upon first presentation was indicative of a “suspicious nodule” in the thyroid gland.
Final Diagnosis
PATHOLOGICAL DIAGNOSIS – excision biopsy of nodule (17/01/2018)
Specimen A: Right lobe of thyroid, hemithryoidectomy: Encapsulated follicular variant of papillary thyroid carcinoma Specimen B: Right cervical lymph node (Level VI), biopsy: Negative for malignancy (0/1)
PATHOLOGICAL DIAGNOSIS – left thyroid lobectomy (11/05/2018):
Left lobe of thyroid, excision: Negative for malignancy
PATHOLOGICAL DIAGNOSIS:
Right thyroid, lobectomy: Negative for malignancy (05/09/2018):
Take Home Messages
Thyroglobulin level is directly proportional to thyroid tissue present in vivo, hence is a useful tumour marker for thyroid cancer.
Anti-thyroglobulin antibody level is tested with Thyroglobulin to exclude false low values of thyroglobulin. If Anti-thyroglobulin Ab levels are increased with a decreased thyroglobulin level, the decrease in tumour marker is likely due to immunological clearance of the thyroglobulin and the result is hence likely false. This is the reason for the following canned text in TrakCare when the thyroglobulin level measures low:
The presence of thyroglobulin antibodies may interfere with the thyroglobulin assay. The result of this test must be treated with reserve if the patient has a positive thyroglobulin antibody test.
TrakCare canned text for low thyroglobulin
Upon total removal of the thyroid, thyroid replacement therapy is necessary, preferably slightly hyperthyroid levels to suppress TSH, and hence prevent tumour growth, as is also evidenced by this patient’s TSH and free T4 results.
As with most other tumour markers, thyroglobulin should be used for follow-up as a proxy of tumour size or regression.
Hyperaldosteronism
HOSP #
WARD
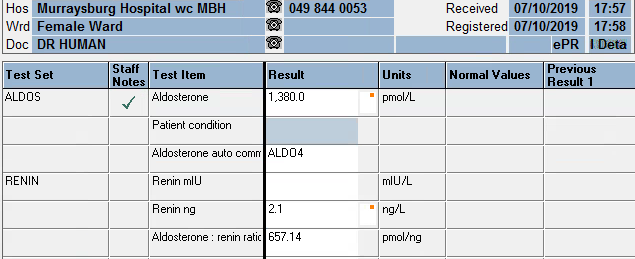
Murraysburg Hospital, Female Ward
CONSULTANT
DOB/AGE
51 y female
Abnormal Result
Aldosterone: 1380 pmol/L
Renin: 2.1 ng/L
Aldosterone: Renin ratio: 657.14 pmol/ng
Presenting Complaint
Uncontrolled Hypertension, unresolved on maximum dose of 3 antihypertensives.
History
Examination
Laboratory Investigations
Other Investigations
Urine electrolytes
Serum Results
Date
Sodium mmol/L
Potassium mmol/L
eGFR ml/min
GGT U/L
Chol mmol/L
TSH mIU/L
T4 pmol/L
FreeT3 pmol/L
Cort nmol/L
21/04/2015
2,8
>60
5,07
30/11/2015
3,8
>60
4,53
15/11/2016
>60
4,04
20/03/2017
>60
4,36
05/06/2018
144
3,4
56
4,39
1,79
11,9
5
394
20/08/2018
131
4,6
42
21/08/2018
24/08/2018
26/08/2018
26/08/2018
26/09/2019
139
2,4
45
0.81
27/09/2019
142
2,6
43
01/10/2019
02/10/2019
139
2,9
40
CEGK
03/10/2019
07/10/2019
138
3,9
38
31/10/2019
139
1,9
30
28
Urine metanephrines
Urine collection period
24 h
Reference value
Urine volume
3080 ml
Ucreat
2,2 mmol/L
Umetadren
160 nmol/L
Unormetadren
870 nmol/L
dUmetadren
493 nmol/24h
152-913
dUnormetadren
2680 nmol/24h
699-2643
Umetadren:cr
73 nmol/mmol creat
17-91
Unormetad:cr
395 nmol/mmol creat
75-309
Final Diagnosis
Primary hyperaldosteronism causing secondary hypertension with accompanying renal injury.
Take Home Messages
Reference Ranges for Aldosterone:
Upright 70 – 1066 pmol/L
Supine 49 – 643 pmol/L
Screening for primary hyperaldosteronism: most sensitive when >350 pmol/L
Reference Ranges for Renin:
Upright: 2.7 – 27.7 ng/L
Supine: 1.7 – 23.9 ng/L
Beta-blockers suppress renin levels and should be stopped 2 weeks before testing.
Aldosterone: Renin Ratio:
Most sensitive when the ratio is >118 pmol/ng.
Effects of hyperaldosteronism
One’s expectation is a high serum sodium, but since it normalizes with an increase in fluid volume, hence hypertension as in this case, there is normal sodium.
Low serum potassium due to loss in urine, although this can also be normal.
Increased urine potassium concentration (>30 mmol/L) in a random urine specimen suggests increased mineralocorticoid effect.
The renin:aldosterone ratio is used to compensate for the increase in aldosterone which is caused by an increase in renin (for instance which is caused by hypovolemia or low blood pressure).
Some studies recently published are suggesting that the prevalence of hyperaldosteronism are significantly more than was (and is) thought, and hence urinary (24 hour) aldosterone measurement may be more accurate to screen for hyperaldosteronism. The authors of recent estimates of the prevalence of hyperaldosteronism are of opinion that hyperaldosteronism may be the cause of around 10% of unexplained “essential” hypertensives (see attached articles).
Above results do not make sense for a 33 year old female, except if muscle weight is extremely low.
History
Examination
N/A
Laboratory Investigations
Inspection of the sample:
On inspection of the sample it is clear that there is dilution with a clear fluid and the hematocrit is affected severely (also visible on results below).
Other Investigations
Lactate on analyser as done on serum sample: >22 mmol/L, dilution made: 1 in 10 revealed a lactate of 26.8 mmol/L in the sample. This could explain that Ringers Lactate was the contaminant in the sample, but can only be hypothesized with the available evidence.
Hematology results:
From the previous (and current) Hematology results available, it is clear that, since all values are lower than the previous day, drip line contamination is the likely cause of the low Chemistry and Hematology results.
Final Diagnosis
Take Home Messages
Loading Viewer...
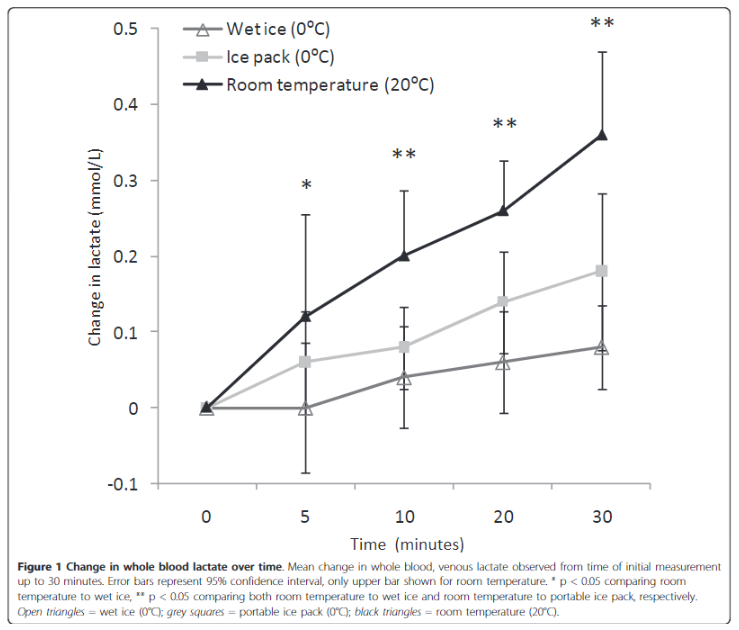
Lactate cannot be measured in SST (serum separator tubes) without taking into account the fact that the red cells will continue to metabolize the glucose in the sample to lactate via anaerobic metabolism through glycolysis.
Lactate concentration increases linearly over time, in whole blood. Factors affecting the rate of production are, among others:
Temperature
Glucose concentration
Additives in the blood tubes such as NaF
NaF inhibits enolase, an enzyme acting late in the glycolytic pathway, and has no effect on enzymes that act early in the glycolytic pathway. … Glycolysis is instantly inhibited in erythrocytes, leukocytes and platelets when the blood pH is maintained between 5.3 and 5.9 with a citrate buffer.
Sage Journals: Ann Clin Biochem 2013;50: 3–5. DOI: 10.1258/acb.2012.012135
Loading Viewer...
Albumin Assay – Bromocresol Green method
Practical Documentation:
Aims
To perform serum albumin determinations on samples, explain the principle behind the Bromocresol Green method for albumin measurement and to list the factors that will cause interference with this method.
Principle
Albumin is known for its ability to bind many types of organic compounds, including organic dyes. When albumin selectively binds with Bromcresol Green (BCG) it causes a change in the absorbance maximum of BCG. The intense blue-green complex that is formed has an absorbance max of 670nm. Bromocresol reagent at pH 4.3 is negatively charged. The pI of albumin is 4.7.
For all spectrometric assays, always use a Reagent
blank. It usually contains all diluents and reagent in the reaction
solution, but no sample. Some reagent blanks do contain the sample as well, but
they lack one crucial reagent component needed to produce a colour-yielding
reaction. This is different from the water used to zero a spectrophotometer
(set 100% T).
Generate a calibration curve of
at least 8 standards (0- 80 g/L) by diluting the Albumin Stock (100 g/L).
In labelled tubes, set up a
calibration, controls and test samples as follows:
Sample
Water (µL)
Std (µL)
Control (µL)
Sample (µL)
BCG Reagent (µL)
Blank
310
–
–
–
300
Calibrators
300
10
–
–
300
Control
300
–
10
–
300
Serum Sample
300
–
–
10
300
Figure 1. Setting up the standards for the calibration curve.
To set up a standard curve with more points along the usable range, I chose more points in the concentration range 20 – 40 g/L, which in my experience constitutes the bulk of albumin measurements.
3. Mix well read immediately at 630nm and record absorbances
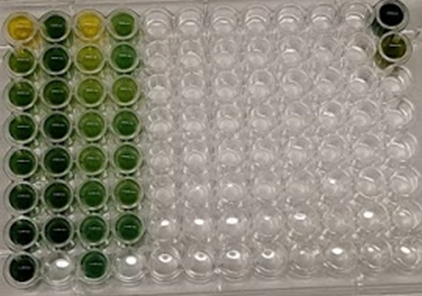
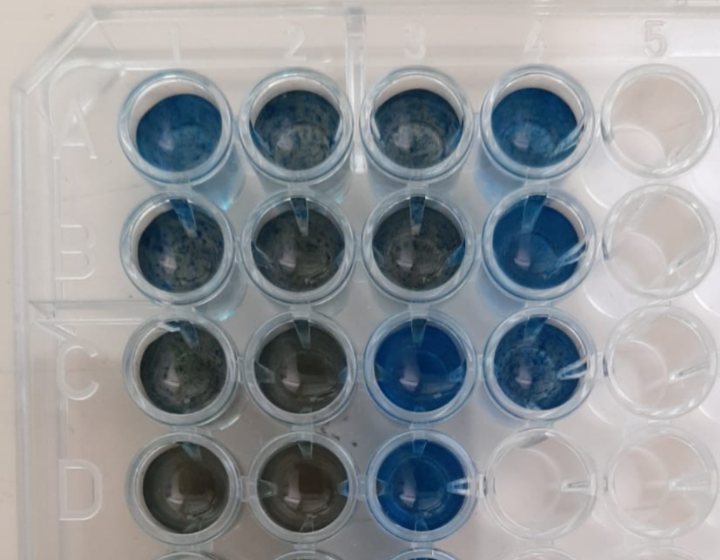
Layout of wells
Dilution as per manual
Dilution of 1:2 with H2O
1
2
3
4
A
Standard 0
Unknown 1
Standard 0
Unknown 1
B
Standard 1
Unknown 2
Standard 1
Unknown 2
C
Standard 2
Unknown 3
Standard 2
Unknown 3
D
Standard 3
Unknown 4
Standard 3
Unknown 4
E
Standard 4
Unknown 5
Standard 4
Unknown 5
F
Standard 5
QC Low
Standard 5
QC Low
G
Standard 6
QC High
Standard 6
QC High
H
Standard 7
Standard 7
Layout of wellsLayout of wells
Absorbance
Absorbance
Standard concentration (g/L)
No dil
Dil 1:2 (150uL reagent mix + 150uL H2O
0
0.095
0.065
20
0.506
0.245
25
0.719
0.345
30
0.779
0.395
35
0.784
0.411
40
0.999
0.504
50
1.242
0.593
80
1.477
0.68
4. Plot a standard curve and determine experimental concentrations of controls and serum samples
Figure 2 – Deriving the formula was done with a statistical Calculator by entering the respective X- and Y-values into a table and obtaining a slope and y-intercept by linear regression. Only the neat reagent mix’s formula was done manually with a calculator. Slope (b) was calculated to be 0.01769 and y-intercept (a) was 0.206. These values corresponded to the values when plotting an X-Y plot on Microsoft Excel (see 2 standard curve data plots above).
The figure below illustrates the formula used to determine the unknown concentrations.
Unknown concentrations were calculated as follows:
Unknowns Sample no.
Absorbance
Absorbance (Diluted 1:2)
Calculated concentration
Calculated concentration (Diluted 1:2)
Reference albumin values (from Roche Cobas 6000)
1
0.893
0.48
Hemolysed
38.8
44.2
29.1
2
1.057
0.55
48.1
53.0
44.2
3
0.614
0.334
23.1
26.0
22
4
0.997
0.5
Hemolysed
44.7
46.7
38.6
5
0.894
0.479
38.9
44.1
33.2
Lo
0.843
0.453
36.0
40.9
31.9
Hi
1.161
0.593
54.0
58.4
49.4
Compare results to expected results and comment on any differences between the manual BCG vs automated BCP assays.
Figure 3 – Manual BCG method vs. Automated BCP method (Roche). It can be seen that the manual BCG method overestimated the albumin concentration in all serum samples. A possible explanation for this difference is: 1. Pipetting error 2. Interferring substances in the serum which absorb light at 670nm. 3. It may be due to the fact that albumin stock solution was made up with water as opposed to physiological albumin-free serum matrix. 4. Hemolysis – Evidenced by one of the hemolysed samples which clearly measured falsely high.
A haemolysed sample is brought to the laboratory for albumin analysis. Can the sample be used? Discuss.
Yes. Hemoglobin does not absorb light at 670 nm, therefor will not interfere significantly with the analysis. See figure below:
It does however interfere in the following manner:
Hemoglobin decreases the apparent albumin concentration by 1 g/L for each 100 g/L added. Blanking does not correct this interference, and the negative bias is therefore caused by interference with the dye binding rather than hemoglobin color. For the BCP method, a blank correction is required on icteric sera and on grossly hemolyzed and grossly lipemic sera to correct for an underestimation of albumin caused by these agents. Heparin causes a positive interference with BCP and BCG methods. This interference can be eliminated by the addition of hexadimethrine bromide to a concentration of 50 mg/L in the BCP reagent
Kaplan’s Methods
Why is it not desirable to incubate the reaction before measuring the absorbance?
Incubating the sample can give rise to other non-specific binding of analytes in the sample to the chromophore dye and a falsely elevated reading can be obtained.
Some analyzers can measure the absorbance of the BCG reaction within 30 seconds after adding sample. Does this tend to increase the specificity of the reaction?
Yes. The less time there is for other interfering substances to bind to BCG, potentially the more specific it will be to albumin, as albumin is the more specific binding to BCG.
Probably the most promising adaptation of the BCG reaction for albumin analysis utilizes fast reaction readings. Gustafsson reported that measuring the absorbance of the BCG-protein complex at 629 nm at a time shortly after mixing improves the specificity of the assay. Interference by other proteins such as ceruloplasmin and orosomucoid becomes significant at times greater than 5 minutes.
Kaplan’s Methods
Total Protein assay – Bradford
Practical 3 : PROTEIN ASSAY- BRADFORD Total /100
INTRODUCTION The Bradford protein assay, is a spectrophotometric assay that is more popular for protein concentration determination than other known protein assay such as the Lowry assay. The Bradford assay is simple, more sensitive and faster than other protein assays (Kruger, 2009). This assay is an example of a dye-binding assay and the dye used is Coomassie Brilliant Blue G-250 (Bradford, 1976; Becker, Caldwell and Zachgo, 1996; Kruger, 2009; Nouroozi and Noroozi, Moulood Valipour Ahmadizadeh, 2015). The principle of this assay relies on the physical interaction of the dye and protein in solution and results in an observable change in colour. The colour change is as follows; red (Amax 465 nm), when not bound to proteins and blue (Amax 595 nm) form of the dye carries a (-) charge and interacts with (+) charges on proteins to form a complex (Becker, Caldwell and Zachgo, 1996).
OBJECTIVES 2.1. To prepare standards through a series of dilutions 2.2. To measure the unknown concentration of a protein in solution via a spectrophotometer 2.3. To analyse, interpret results about CV%, SD, LOD and LOQ.
PROCEDURES A. PREPARATION BEFORE THE PRACTICAL Complete the following BEFORE your practical session: • You would need to do some extra reading on the Bradford protein assay and spectrophotometer principles (i.e. Beer Lambert law) in preparation for your practical and test. • Find and print SDS’s for the following chemicals; Tris (trisaminomethane), Hidrochloric acid (HCL), ethanol, Phosphoric acid and Coomassie Brilliant Blue G-250. • Prepare a practical plan for your experiment that you will be conducting today.
B. PRACTICAL SESSION (Total 50) Complete the following DURING your practical session: (1) Complete the practical test. (2) Using the Bradford Assay determine as follows: Materials provided: • Tris buffer: 10 mM Tris-HCl (pH 7.0)] • Bovine serum albumin (BSA) stock solution: [2 mg/ml BSA in Tris buffer (pH 7)] • Bradford reagent; [0.01% (w/v) Coomassie Brilliant Blue G-250, 4.7% (w/v) ethanol, 8.5% (w/v) phosphoric acid] • Unknown protein sample
Method: a) In Eppendorf tubes, prepare a series of BSA solutions of varying concentration by diluting the 2 mg/ml BSA stock solution with Tris-HCL buffer (You will need ~200μL of each dilution) to set up a calibration curve (at least 7 concentrations to be used).
Serial dilutions were made in 1.5mL Eppendorf tubes:
Standard no.
Protein concentration (ug/ml)
1 (500uL of provided 2ug/ml stock solution)
2
2 (250 uL of S1 plus 250uL Tris-HCl diluent)
1
3 (250 uL of S2 plus 250uL Tris-HCl diluent)
0.5
4 (250 uL of S3 plus 250uL Tris-HCl diluent)
0.25
5 (250 uL of S4 plus 250uL Tris-HCl diluent)
0.125
6 (250 uL of S5 plus 250uL Tris-HCl diluent)
0.0625
7 (250 uL of S6 plus 250uL Tris-HCl diluent)
0.03125
8 (Also Blank – Only 250uL Tris-HCl)
0
Standard preparations.
b) Add 2.5 mL of Bradford reagent to a separate cuvette for each of your samples and label them appropriately. Consider the value of determining the concentration of one or more dilutions of your unknown sample as well as the undiluted (“neat”) unknown sample.
To save cuvettes, I have used an old refurbished microtitre plate with 10x less volume, hence 250uL
c) Prepare your samples by adding 50μL of each protein sample (diluted standard or unknown) separately to the Bradford reagent in the appropriately labelled tube. Mix the tubes by gentle inversion several times, and let the colour develop for 5 min. Observe and record the colour change of your standard samples as a function of protein concentration. A blank sample is prepared by mixing 50μL Tris buffer with 2.5 ml Bradford reagent.
As above, to save reagent and test my pipetting skills, I have used 5uL as one set of additions and also made a 1:1 (2x) dilution of my standards to run another calibration curve. The unknown sample was also added as neat and a 2x dilution.
d) You will need to determine which portion of the UV/vis spectrum, specifically which wavelength will be useful for following the dye bound by protein. Take a full spectral scan of your Bradford reagent blank. When your standard samples have fully developed, take a full spectral scan of the most concentrated standard you prepared.
Fig. 1 – Wavelength scan of the reagent blank as well as the Highest standard after full colour development.
e) Based on your results, choose a single wavelength suitable to analyse the results of your dye-binding assay. Measure and record the absorbance of each standard and unknown sample at your chosen wavelengths using cuvettes.
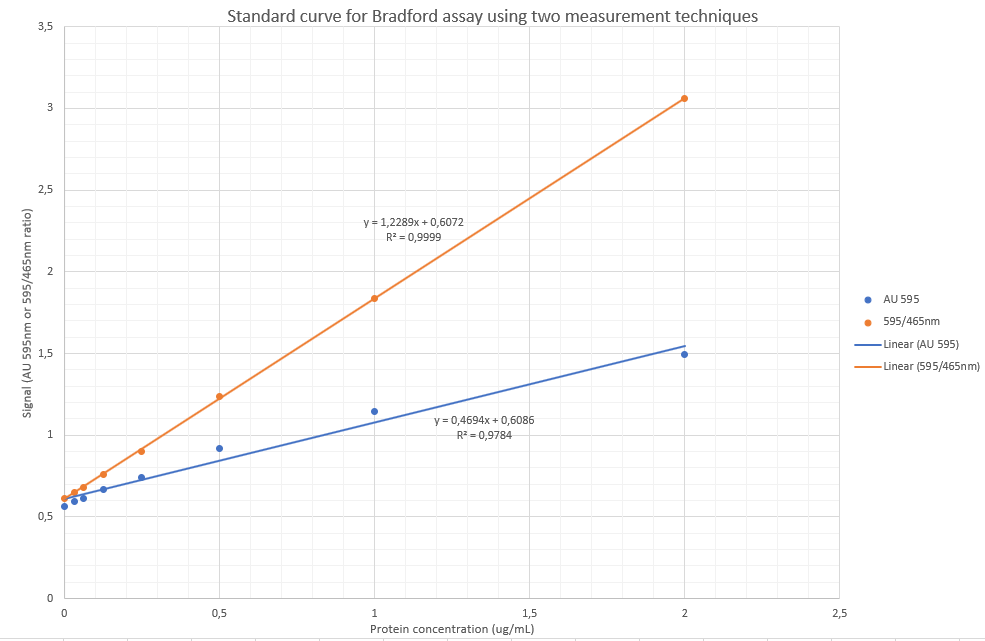
From above wavelength scan it is evidenced that the maximum absorbance after colour development occurs at 595 as published widely in the literature for the Bradford assay. I am, however going to perform a slight variation also published before, by using the ratio of absorbance 595nm/465nm as the signal, as it has before been shown to be more sensitive. The rationale thereof is that there is reduction of absorbance intensity at 465nm and increase of intensity at 595nm, hence likely causing slight increases in sensitivity and arguably a more accurate assay.
f) At your determined wavelength, read your unknown sample at approximately every 10 minutes for 1 hour, you will use these readings to calculate the percentage (%) change over time.
Fig. 2 – To calculate the %change over time is relatively simple by using the slope of the linear regression line: If using the orange line’s formula at 595nm only: slope = – 0.0081, which means that the absorbance values decreases in general by 0.0081 AU per minute. This is, however subject to variability as the reagent/protein complexes was observed as precipitating out and the final portion of the curve (after 50 min) is likely not fitting due to this phenomenon. Nevertheless, using a decrease of 0.0081AU per minute, means that at an absorbance value of 1.25 (top of the calibration curve), 0.0081/1.25*100 = 0.65% decrease in absorbance per minute.Fig. 3 – Indication of precipitation happening after an hour of incubation.
g) Prepare your highest standard in five (5) cuvettes and read the absorbances of each cuvette two times, so in total you will have 10 readings. These results you will use to calculate the protein concentrations and then calculate the CV% and SD
h) Make sure your lab space is clean and disinfected.
C. AFTER PRACTICAL SESSION Complete the following for submission before or during the next practical Answer the following questions:
QUESTION 1 (Total 15) Using the resulting equation for the calibration curve, determine the protein concentration of your unknown sample.
Prot. Conc
Abs 595
465nm
595/465 ratio
2
1,4949
0,488
3,06332
1
1,146
0,6248
1,834187
0,5
0,9158
0,7388
1,239578
0,25
0,7401
0,8203
0,902231
0,125
0,6648
0,8788
0,756486
0,0625
0,6138
0,9023
0,680262
0,03125
0,5932
0,9143
0,648802
0
0,5633
0,9234
0,610028
Table 1 – Absorbance values obtained
To determine the unknown:
Via AU595nm:
y=0.4694x + 0.6086
x= (y-0.6086)/0.4694
x= 1.34g/L
Via the 595/465nm ratio:
y = 1.2289x + 0.6072
x=(y-0.6072)/1.2289
x= 1.25g/L
QUESTION 2 (Total 10) Calculate the percentage (%) change over time of your unknown sample and comment on the stability of your assay.
Referring to Fig. 2 – To calculate the %change over time is relatively simple by using the slope of the linear regression line: If using the orange line’s formula at 595nm only: slope = – 0.0081, which means that the absorbance values decreases in general by 0.0081 AU per minute. This is, however subject to variability as the reagent/protein complexes was observed as precipitating out and the final portion of the curve (after 50 min) is likely not fitting due to this phenomenon. Nevertheless, using a decrease of 0.0081AU per minute, means that at an absorbance value of 1.25 (top of the calibration curve),
0.0081/1.25*100 =
0.65% decrease in absorbance per minute.
The stability of the assay is likely around 15-20 minutes.
QUESTION 3 (Total 15) Calculate the CV% and SD using your data.
Absorbance Value
Calculation
1.6096
1.6124
1.5923
1.5345
1.498
1.5602
1.5624
1.5425
1.4823
1.4567
Stdv
0.050538
Mean ( (Sum of values)/n)
1.54509
CV%
3.270859 %
Calculation of mean absorbance and CV on the highest standard.
QUESTION 4 (Total 10) Calculate the LOD, LOQ, and comment on the linearity of your assay.
Using only the 595nm absorbance yielded a poor result (r=0.9784).
Using the 595/465 ratio, the linearity was much better (r = 0.9999)
SE of intercept: Excel Function: STEYX(X-values;Y-values)
LOD = 3.3 * (SD of intercept / slope)
LOQ = 10 * (SD of intercept / slope)
Prot. Conc
Abs 595
465nm
595/465 ratio
2
1,4949
0,488
3,06332
1
1,146
0,6248
1,834187
0,5
0,9158
0,7388
1,239578
0,25
0,7401
0,8203
0,902231
0,125
0,6648
0,8788
0,756486
0,0625
0,6138
0,9023
0,680262
0,03125
0,5932
0,9143
0,648802
0
0,5633
0,9234
0,610028
AU595 only
Slope
0,469384
STEYX
0,052252
LOD
0,367358
ug/mL
LOQ
1,113206
ug/mL
595/465 ratio
Slope
1,228876
STEYX
0,051192
LOD
0,137467
ug/mL
LOQ
0,416565
ug/mL
Table 2 – Limit of detection (LOD) and limit of quantification (LOQ) between the different measuring procedures.
REFERENCES: Becker, J. M., Caldwell, G. A. and Zachgo, E. A. (1996) ‘Protein Assays’, in Biotechnology. Elsevier, pp. 119–124. doi: 10.1016/b978-012084562-0/50069-2. Bradford, M. M. (1976) A Rapid and Sensitive Method for the Quantitation of Microgram Quantities of Protein Utilizing the Principle of Protein-Dye Binding, ANALYTICAL BIOCHEMISTRY. Kruger, N. J. (2009) ‘The Bradford Method For Protein Quantitation’, in The Protein Protocols Handbook. Humana Press, Totowa, NJ, pp. 17–24. doi: 10.1007/978-1-59745-198-7_4. Nouroozi, R. V. and Noroozi, Moulood Valipour Ahmadizadeh, M. (2015) ‘Determination of Protein Concentration Using Bradford Microplate Protein Quantification Assay’, International Electronic Journal of Medicine, 4(1), pp. 11–17. doi: 10.31661/iejm158.
1 day of poor feeding. Child passing very hard/ dark brown stool for the preceding 10 days.
History
Birth weight @ term: 3.380kg. Delivered vaginally after induction of labour because of spontaneous rupture of membranes at 40 weeks gestation. Discharged home without any problems after 1 day.
Examination
On arrival at district hospital: Temp: 38oC, Sats 96% on Nasal O2, Finger prick glucose: 10mmol/L, Capillary refill time: 6 seconds,
Urine organic acid analysis by GCMS demonstrates elevation of the liver markers 4-OH-phenyllactate and 4-OH-phenylpyruvate together with lactaturia. Succinylacetone, a marker for tyrosinaemia type 1 is absent. Moderate ketonuria with elevated dicarboxylic acids C6, C8, and C10 is also present, these changes suggest a lipolytic response to catabolic or fasting stress or hypoglycaemia together with underlying hepatic dysfunction with lactataemia but are non-specific for an IMD per se.
Final Diagnosis
Patient was pure water depleted with a sodium concentration of 198 mmol/L. The mother was not lactating adequately despite the infant sucking well, evidenced by the fact that when expressed breast milk was tried, there was too little milk for the baby to drink. The nurses’ notes confirmed this finding. This finding also confirms the failure to produce stool volume and the normal urine organic acid profile with evidence of starvation / fasting stress.
Take Home Messages
When considering a patient with high plasma sodium concentration it is
important to bear in mind:
Hypernatremia does not necessarily indicate an excess of extracellular sodium. Except in rare cases of salt overload most patient with hypernatremia have a deficiency of both water and sodium, with the water deficiency being proportionally higher than that of sodium.
Patients become hypernatremic because the water lost from the body exceed the intake and there is negative fluid balance. The amount of water which a person can drink generally exceeds by far the amount lost from the body in most pathological fluid-losing disorders, eg. Diarrhoea, sweating. Patients thus become hypernatremia due to:
Too old, young or sick to drink
Obstruction of oesophagus
Disorders of thirst centre
No access to water
Ref: Walmsley – Cases in Chemical Pathology 4th ed.
It is also important:
To calculate the Osmolar gap( difference between calculated and measured osmolarity)
U:P osmol (>1 = hypotonic fluid depletion, pure water loss or salt gain; ~1 = osmotic diuresis; <1 = diabetes insipidus ~the various causes of nephrogenic and neurogenic DI)
Prolactin
HOSP #
WARD
ENT Clinic
CONSULTANT
DOB/AGE
35 Y Male
Abnormal Result
Prolactin 10 986.0 ug/L (4-15.2)
Dilutions:
1/10 >4700;
1/100 = 10821;
1/50 = 10 986.
Presenting Complaint
Epistaxis
History
Patient with epistaxis referred to the ENT specialist clinic. No relevant medication history.
Examination
35 y male with a large left post-nasal space mass, a vascular mass involving the pituitary fossa.
?NBL (non-benign lesion)
?Sinonasal malignancy
?Pituitary Tumour
Laboratory Investigations
TSH 0.91 pmol/L (0.27-4.20)
Free T4 15.7 pmol/L (12-22)
FSH 0.8 IU/L ↓ (1.5-12.4)
LH 0.2 IU/L ↓ (1.7-8.6)
Testosterone 0.2 nmol/L ↓ (8.6-29.0)
PTH 1.7 pmol/L (1.6-6.9)
Prolactin measuring method:
The Elecsys prolactin sandwich immunoassay uses two monoclonal
antibodies directed against human prolactin.
R1 = biotinylated antibody – recognizes the N-terminal end of the
prolactin molecule
R2 – ruthenium complexed antibody probably reacts with a region in the
middle of the prolactin molecule.
1st incubation: a biotinylated monoclonal prolactin-specific
antibody and a monoclonal prolactin-specific antibody labeled with a ruthenium
complex form a sandwich complex.
2nd incubation: after addition of streptavidin-coated
microparticles, the complex becomes bound to the solid phase via interaction of
biotin and streptavidin.
Reaction mixture aspirated into the measuring cell where microparticles
are magnetically captured into the surface of the electrode. Unbound substances are then removed with
ProCell.
Application of a voltage to the electrode then induces
chemiluminescent emission which is measured by a photomultiplier, results
calculated by a standard curve.
Other Investigations
Monomeric prolactin – 7744 ug/L (70% recovery after PEG precipitation)
Biopsy: confirmed tumour stained strongly positive
with prolactin suggesting a prolactinoma.
Final Diagnosis
Pituitary Macroprolactinoma
Take Home Messages
Sandwich immunoassays are prone to high dose hook-effect. There are
various ways to overcome this effect. (This will later be expanded on – see AFP
/ Beta-HCG).
Precipitation by PEG yields the active monomeric
prolactin, expressed as a percentage recovery after precipitation. Big-big prolactin consists of an
antigen-antibody complex of monomeric prolactin-immunoglobulin G and is defined
as macroprolactin. This has a long
half-life in blood when compared to normal prolactin and gives false high
readings of prolactin, leading to unnecessary investigations in certain
cases. A high prolactin should thus be
confirmed by doing a PEG precipitation.
Fluid Triglycerides
HOSP #
WARD
Surgical ICU
CONSULTANT
Dr. Heleen Vreede
DOB/AGE
23y Female
Abnormal Result
Fluid triglycerides were requested on three samples, without any clinical information.
Presenting Complaint
The laboratory history was explored, to find that the patient had three subsequent samplings daily from a pleural fluid cavity.
History
A month prior to presentation, the patient had a breached stillbirth.
The following was found on Histology:
EPISODE NUMBER:
SA03381462
CLINICAL DETAILS:
23 year old female. G02 P2-1. VDRL: negative. Smoking: 8/day. Alcohol: none. HIV: negative. 750g breech stillbirth at 28/40.
MACROSCOPY:
The plate measures 130 x 100 x 30mm and weighs 196.8g.
The membranes are complete without evidence of meconium staining.
The cord measures 300mm in length with an average diameter of 15mm. Three umbilical vessels are identified with 3 twists per 100mm. The cord insertion is off-centre, 20mm from the plate margin.
Congested blood vessels are identified on examination of the foetal surface.
Cut-sections of the plate show:
- Retroplacental clot.
MICROSCOPY:
General:
Placental weight for gestational age is below the 10th percentile at 196.8g. Partial autolysis is present throughout the specimen.
The umbilical cord and membranes:
The umbilical cord contains two arteries and one vein. There is no evidence of vasculitis or funisitis. Wharton's jelly and membranes do not show meconium uptake. The amniocytes are intact and show no evidence of vacuolation or hyperplasia.
Chorionic plate:
The chorionic plate vessels are focally dilated. There is no evidence of chorioamnionitis.
Villi and intervillous spaces:
The stem villous vessels show partial obliteration as well as stromal sclerosis. Distal villous hypoplasia as well as accelerated villous maturation is seen. Intervillous thrombi are seen as well as intraparenchymal extension of the retroplacental haematoma. There is no evidence of infarction, villitis or intervillositis.
Maternal surface:
There is evidence of a large retroplacental haematoma. No chronic deciduitis or untransformed blood vessels are seen.
PATHOLOGICAL DIAGNOSIS:
Placenta, examination:
Maternal vascular malperfusion.Retroplacental haematoma.
Reported by: Dr M Du Toit
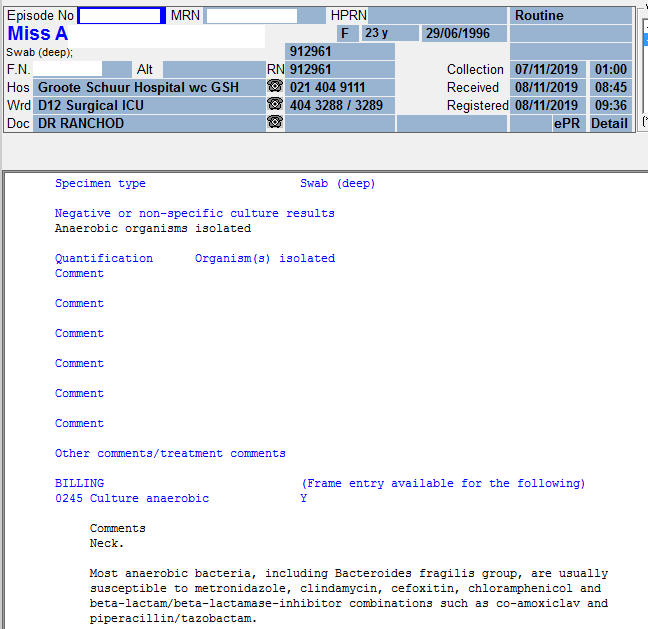
Clinicians were indeed querying a chylothorax. A thoracic duct injury was suspected.
Examination
Unfortunately little clinical information is known, as can be seen above. The following table shows the clinical info which has been captured on the respective episodes’ request forms:
A pleural fluid triglyceride >1.24 is suggestive of chylothorax.
The additional finding of a thin white layer present on the top of the sample after centrifugation indicates the presence of chylomicrons in the sample, which further supports the diagnosis of chylothorax.
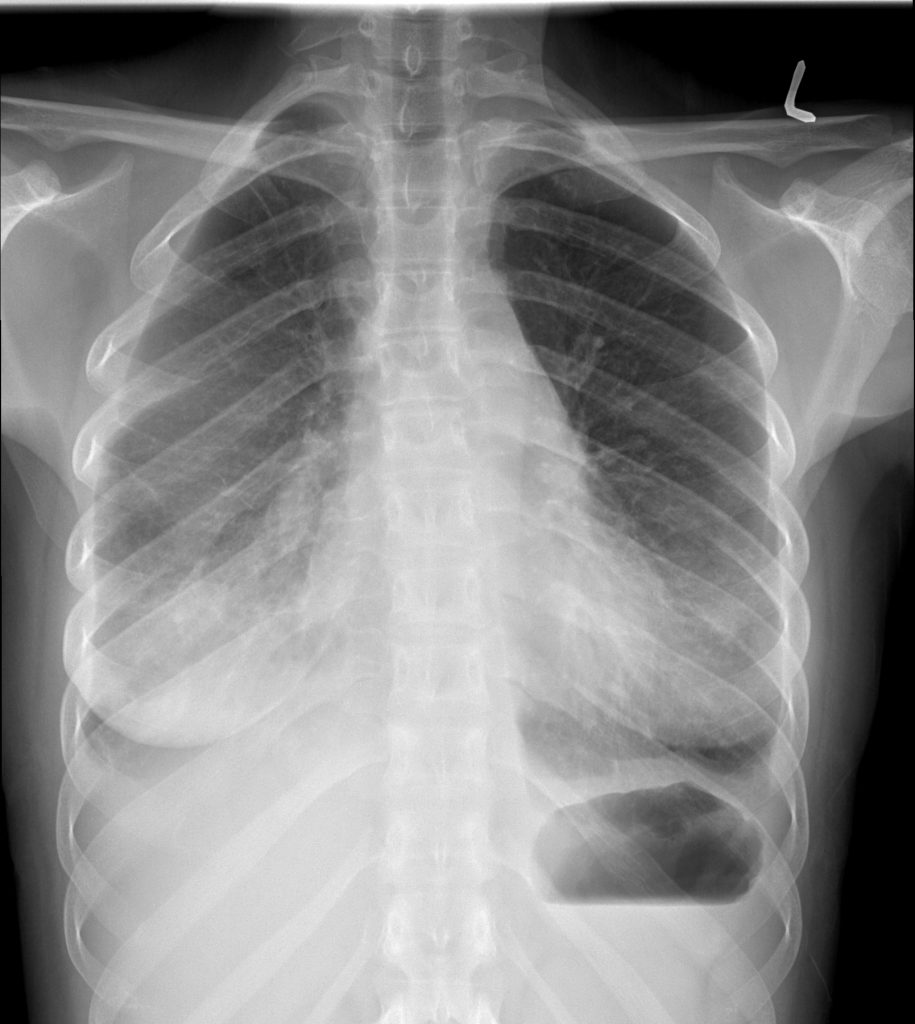
Neck X-ray on 06/11/2019Chest X-ray PA 06/11/2019Chest X-ray lateral 06/11/2019CT chest 11/11/2019 CT chest 11/11/2019CT scan on 11 November 2019Chest X-ray 12/11/2019Chest X-ray 12/11/2019Chest X-ray Mobile 14/11/2019
Take Home Messages
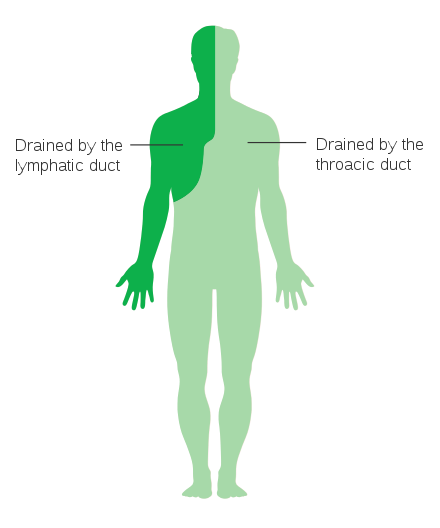
The primary role of the thoracic duct is to carry 60 – 70% of ingested fat at a concentration of 0.4 – 6 g/dl from the intestine to the circulatory system.
Chyle contains large amounts of cholesterol, triglycerides, chylomicrons and fat soluble vitamins.
Lymph is the other main constituent of chyle and is made up of
immunoglobulins
enzymes
between 400 and 6800 white blood cells/ml, the majority of which are lymphocytes.
Chyle transportation is maximal after a high fat meal and minimal with starvation where flow is reduced to almost a trickle.
Classically, a chyloma, a collection of chyle below the pleura develops when the thoracic duct first leaks. Although rarely detected, it manifests itself as a swelling in the supraclavicular fossa which may be associated with severe chest pain, dyspnoea and tachycardia.
Chylomas can also manifest themselves at other sites of the pleura without causing supraclavicular swelling. Eventually the chyloma bursts through the pleura where the chyle accumulates in the pleural space.
Very rarely, the chyle leak may lead to chylomediastinum or chylopericardium.
Roughly 2.4 l of chyle is transported through the lymphatic system every day.
Damage to, or rupture of the thoracic duct can give rise to a large and rapid accumulation of fluid in the pleural space.
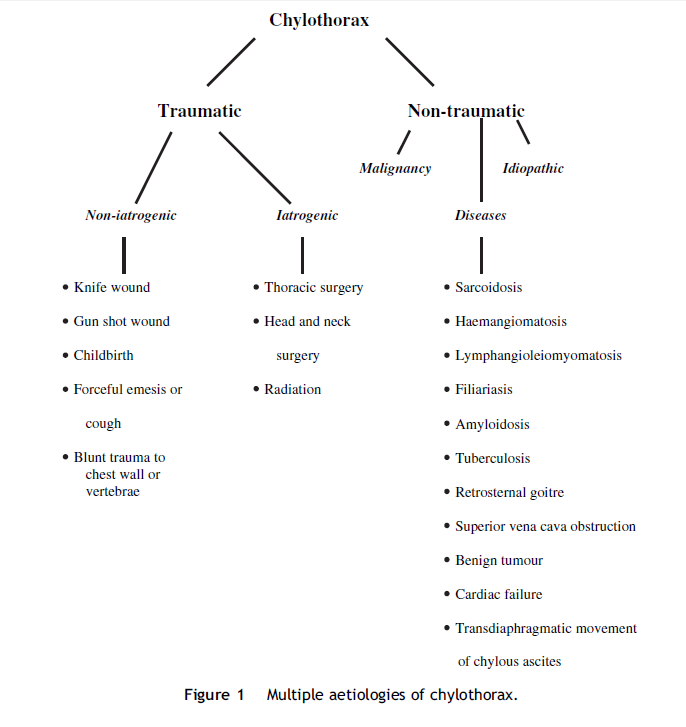
Causes of chylothorax can be classified as follows:
The theorized causes of chylothorax in this case could be one of the following:
The breached stillbirth a month prior to presentation could have caused rupture of the thoracic duct due to increased pressure due to extreme valsalva. Could this be dormant for 1 month and then present with the neck abscess with an anaerobic infection? Could anaerobic bacterial transmission from the gut into a chylous cyst in the neck be the cause? It is however unlikely that delivery of a 750g fetus causes that much trauma.
Iatrogenic chylothorax due to the thoracic surgery.
Left-sided placement of a Central Venous Catheter during delivery of the stillbirth, which accidentally damaged the thoracic duct. The placement of the CVP could also have caused a pneumothorax with subsequent stretching and damage to the thoracic duct.
Remember Chylomicrons float!
ACTH
HOSP #
WARD
G16 Medical Ward
CONSULTANT
DOB/AGE
54 y Female
Abnormal Result
21/08/2018 Two ACTH tests (referred to another laboratory) and two
Cortisol levels (at our laboratory) were done.
At first it was thought to be a dexamethasone suppression test, but then
realized the clinicians were suspecting hypopituitarism.
Known with a pituitary macroadenoma, previously seen at the Radiotherapy clinic in 2016.
Examination
No clinical info available.
For Primary adrenal insufficiency one would expect: Hyperpigmentation
(due to ↑ ACTH), +/- hyperkalemia/hyponatremia (aldosterone effect), +/-
virilization.
For Secondary adrenal insufficiency there is subtle symptoms, electrolytes are not deranged significantly because aldosterone function is preserved. See table on Bishop 7th ed. p. 459.
Laboratory Investigations
Measurement of
plasma ACTH concentration is used to assess Cushing’s disease, adrenal tumors,
ectopic ACTH-producing tumors, Addison’s disease, Nelson’s syndrome, and
hypopituitarism.
The
laboratory diagnosis of hypopituitarism, however is relatively straightforward.
In contrast to the primary failure of an endocrine gland that is accompanied by
dramatic increases in circulating levels of the corresponding pituitary tropic
hormone, secondary failure (hypopituitarism) is associated with low or normal
levels of tropic hormone. This is the
diagnosis in this case with the history of previous radiotherapy which was
given for a macro-adenoma.
Other Investigations
Free T4 on 19/04/2018 was 7.8 pmol/L (12-22), also suggesting possible hypopituitarism, although a TSH would be helpful.
Final Diagnosis
Hypopituitarism confirmed.
Take Home Messages
Dexamethasone suppression test need only measurement of cortisol, not accompanying ACTH, except in extended work-up however, where a Cosyntropin (CRH) stimulation test can be done to distinguish between pituitary or hypothalamic insufficiency.
Evaluation of pituitary function need the Primary hormone (Cortisol) as well as the tropic hormones from the pituitary (ACTH).