A case of severe hypoalbuminaemia
| HOSP # | Lab no: SA03948371 | WARD | Paediatric Ward |
| CONSULTANT | Dr. Jody Rusch | DOB/AGE | 16 y Female |
Abnormal Result
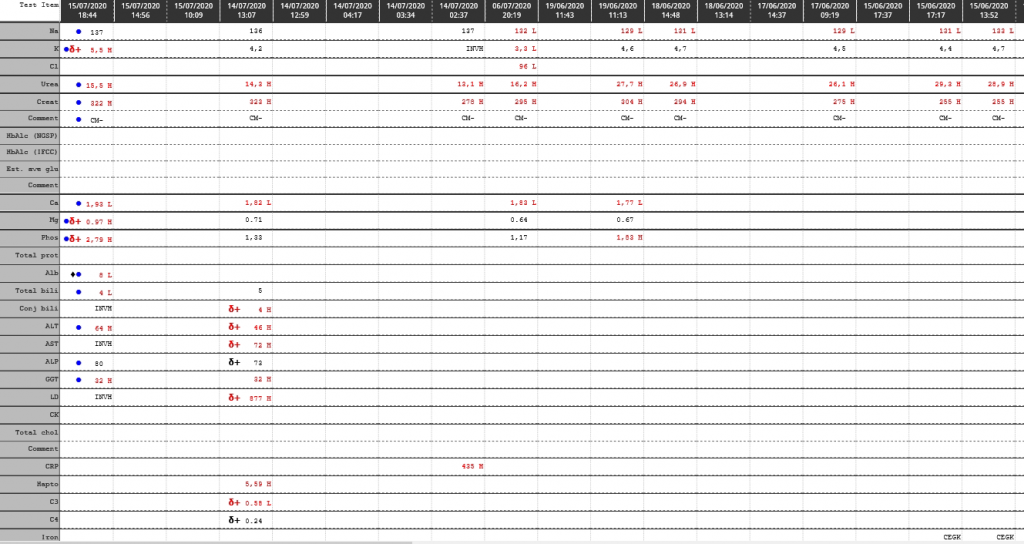
Albumin of 8 g/L
Presenting Complaint
Signs and symptoms of a urinary tract infection made the patient present to a general practitioner.
History
No known chronic medical illness were present upon initial presentation.
No medical treatment was being taken for chronic illnesses.
The patient had reported taking NSAIDS before for pain in the lower abdomen. The exact drug / dose was unknown.
Examination
All clinical findings are unfortunately not available for this patient.
It is known that the patient had been having lower abdominal pains upon presentation (which was not due to pregnancy).
A urinary tract infection was suspected by the initial treating physician. Upon the other finding of edema, investigation towards the cause was investigated.
Typical findings of nephritic syndrome are:
- Fever
- Edema (due to hypoproteinemia)
- High blood pressure (due to activation of the renin-angiotensis-aldosterone system).
- Joint pain
- Muscle pain
- Malar rash
- Foamy urine (proteinuria)
Laboratory Investigations
Albumin 14 g/L
Cholesterol 8.14 mmol/L
Urine Protein:Creatinine ratio: 1.62 g/mmol creat
C3: 0.29 (Low)
C4: 0.07 (Low)
Creatinine 255 – 322 umol/L
Other Investigations
Final Diagnosis
Lupus Nephritis with hypoalbuminemia
Take Home Message
The clinical presentation of this patient is a good example of the findings in patients who initially present with renal failure. The extent of renal failure is often so severe, that when the patient presents with signs and symptoms of renal failure, there are quite significant permanent renal damage already.
Patients with nephrotic syndrome present with significant proteinuria with resultant hypoproteinemia, firstly hypoalbuminemia, followed by the other bigger proteins like gammaglobulins, alpha-1, beta-1 and beta-2 (complement) proteins. Because alpha-2 (macroglobulin) comprises one of the biggest proteins (in molecular size) in the serum, it generally stays in the serum relatively longer than the other leaking proteins.
Because the liver increases its production of proteins to try compensate for the reduction in osmolality, the production of VLDL rises significantly and hence Triglycerides (and cholesterol) rises. Thus cholesterol in this patient measured 8.14 mmol/L.
The pathophysiology of lupus nephritis is that of autoimmunity. Autoantibodies direct themselves against nuclear elements. The characteristics of nephritogenic autoantibodies are antigen specificity directed at the nucleosome. High affinity autoantibodies form intravascular immune complexes, and autoantibodies of certain isotypes activate complement. Hence the C3 and C4 which are low often indicates active lupus disease.