Iron deficiency anemia with a twist
| HOSP # | MRN53499748 | WARD | C15 Emergency Unit |
| CONSULTANT | Dr. Heleen Vreede | DOB/AGE | 16 y/o Female |
Abnormal Result
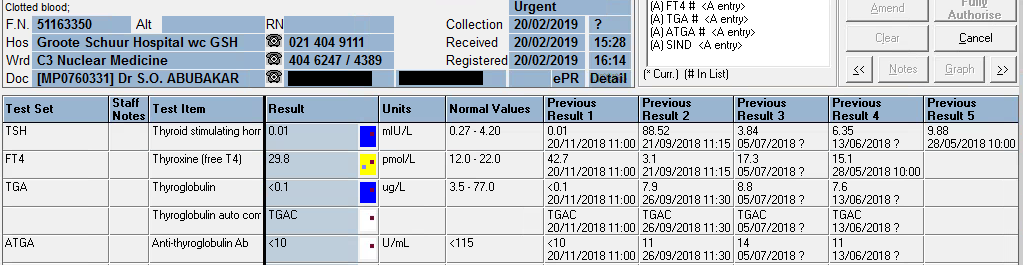
TSH: 42.9 mIU/L (0.51 – 4.30)
Free T4: 7.1 pmol/L (12.6 – 21.0)
Presenting Complaint
Patient presented with signs and symptoms of iron deficiency anemia.
History

The patient is a known hemophilia B carrier (Factor IX deficiency or Christmas disease) with menorrhagia and accompanying iron deficiency anemia.
Examination
The patient presented to the emergency rooms with symptoms of severe weakness and had occasional severe menorrhagia.
Unfortunately the physical examination details are not available.
Laboratory Investigations
- Iron: 4.5 umol/L (9-30.4) Low
- Transferrin 3.92 g/L (2-3.6) High
- % Saturation 5% (15 -50) Low
- Ferritin 8 ug/L (13- 68) Low
Other Investigations
Anti-Thyroglobulin (anti-TG) antibodies as well as Anti-Thyroid Peroxidase (anti-TPO) antibodies were positive in this patient.
These antibodies was suggested after the results of the TSH and reflexed free-T4 became available and hence after-requested.
Final Diagnosis
The pattern of significantly raised TSH with the significantly low free-T4 and the raised anti-TPO and anti-Thyroglobulin antibodies suggest primary hypothyroidism.
Take Home Message
It’s always worth doing a TSH to screen for thyroid disease when a patient presents with weakness / tiredness, irrespective of the age.
Primary hypothyroidism due to an auto-immune mediated destruction of the thyroid gland tissue is the most common hypothyroid condition and is confirmed by measuring the common anti-thyroid antibodies: Anti-TPO and Anti-TG antibodies. There is likely not much indication for performing these antibodies more than once after diagnosis of hypothyroidism and some clinicians argue it not necessary to even perform these antibody measurements.
Congenital hypothyroidism is one of the congenital disorders causing cretinism which is most preventable by newborn screening. Even though not likely congenital in this patient, it’s worth considering on the differential diagnosis.
The patient was on iron supplements as well as Factor IX injections. I was not aware of an association between Factor IX deficiency and Hypothyroidism, but my Haematology colleagues across the corridor told me the following:
Factor IX deficiency is an X-linked recessive disorder. This makes it unlikely for a female to get this disease. Auto-immune diseases is much more likely in females. There is also a form of Christmas disease where one produces antibodies to factor IX, which yields it inactive, hence presenting as Factor IX deficiency.
This, although unlikely, presents an interesting thought for this unusual presentation in this 16-year old female. Acquired deficiencies of most clotting factors have been described.
However, upon discussion with the attending clinician it seems that the patient did have a clear family history of Christmas disease, hence the presentation.