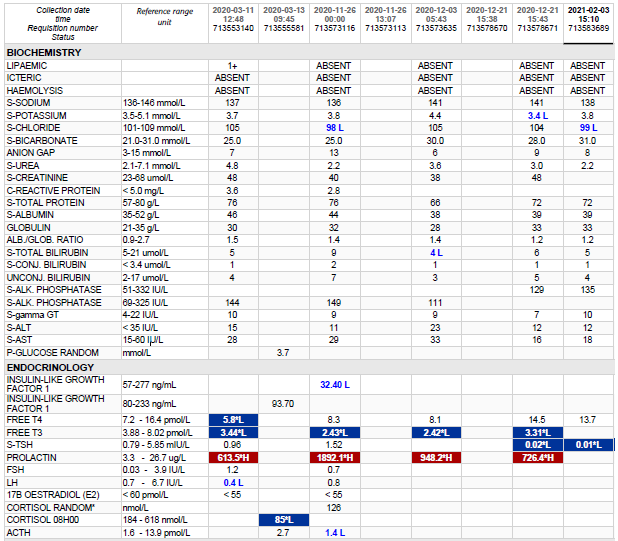
Hyperprolactinemia >1000
| HOSP # | WARD | Neurosurgery | |
| CONSULTANT | Dr. Jody Rusch | DOB/AGE | 10 year female |
Abnormal Result
Prolactin >1000 ug/L
Presenting Complaint
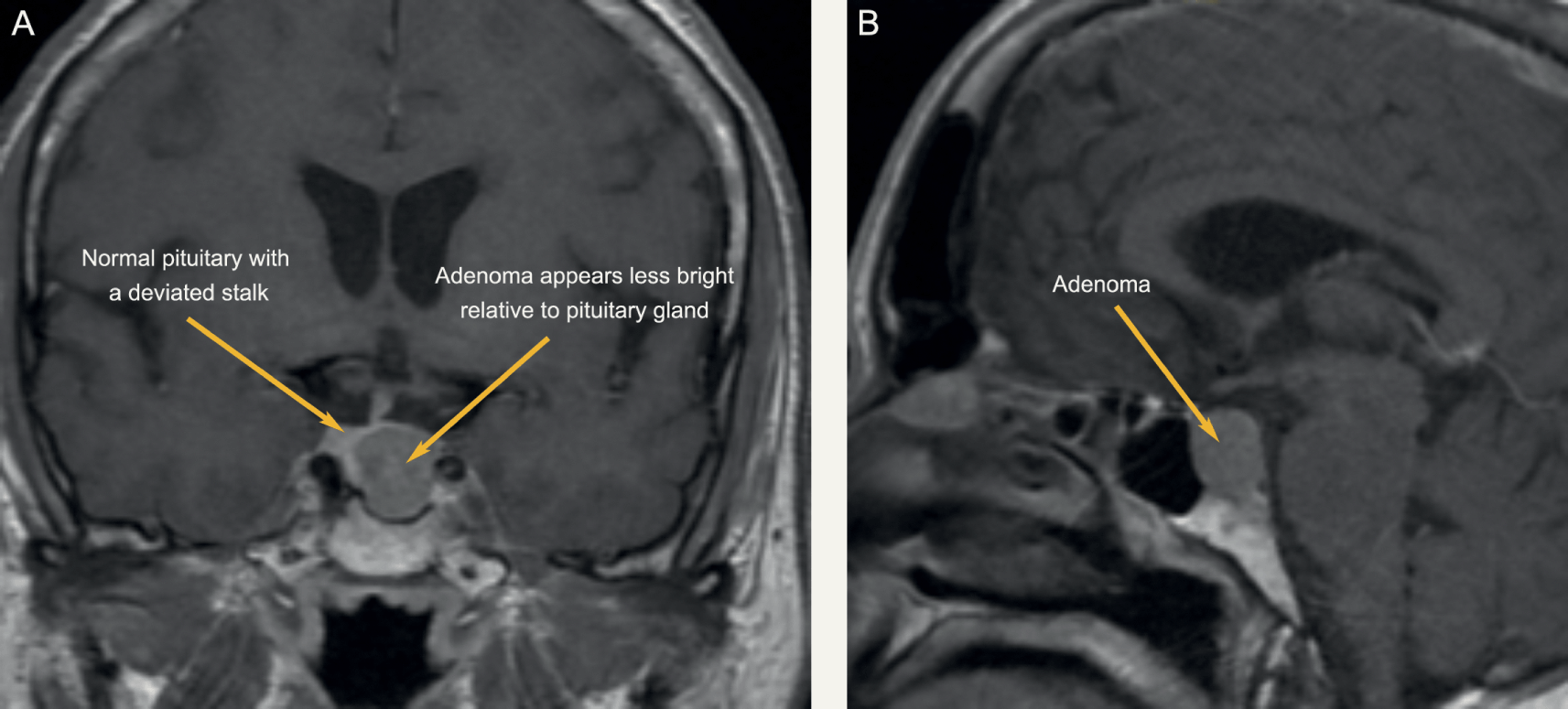
Patient presented at 7 years of age with galactorrhea and visual field defects.
History
Patient had a craniotomy for debulking of the adenoma. This was opposed to the usual transsphenoidal more non-invasive route of pituitary adenoma surgery. She was initiated on Cabergoline 1 g twice weekly for suppression of the tumour size.
It was also noted during surgery that the tumour was extremely vascular with much bleeding and the neurosurgeons struggled to mobilize it to adequately get it separated from the optic chiasm. Some portion of the tumour was left in situ during surgery as this was too big a risk for trying to excise.
A biopsy was also taken.
Examination
Patient subsequently developed severe intracranial edema after surgery in the ICU.
Laboratory Investigations

Other Investigations
Histology
Frozen section – pituitary adenoma. GROSS DESCRIPTION: Specimen labelled tumour. Specimen consists of 2 fragments of tissue, larger measuring 4x3mm. HISTOLOGY: Sections show tumour tissue composed of nests of monotonous cells with intervening fibrous septae. The cells have round nuclei and abundant eosinophilic cytoplasm. The nuclei have stippled chromatin with inconspicuous nucleoli. No mitotic activity or necrosis is seen. Immunohistochemistry: Synaptophysin:Positive Prolactin: Positive LH: Negative FSH: Negative GH: Negative TSH: Negative ACTH: Negative CONCLUSION: Pituitary, mass, excision: – Pituitary adenoma with an immunohistochemical profile compatible with a prolactinoma.
Final Diagnosis
Pituitary Macroadenoma
Take Home Message
Cabergoline, sold under the brand name Dostinex among others, is a dopaminergic medication used in the treatment of high prolactin levels, prolactinomas, Parkinson’s disease, and for other indications. It is taken by mouth. Cabergoline is an ergot derivative and a potent dopamine D₂ receptor agonist.
Lactotroph adenomas (prolactinomas) are more amenable to pharmacologic treatment than any other kind of pituitary adenoma because of the availability of dopamine agonists, which usually decrease both the secretion and size of these tumors. For the minority of lactotroph adenomas that do not respond to dopamine agonists, other treatments must be used. Hyperprolactinemia due to nonadenoma causes should also be treated if it causes hypogonadism.
There are two principal reasons why patients with hyperprolactinemia may need to be treated: existing or impending neurologic symptoms due to the large size of a lactotroph adenoma, and hypogonadism or other symptoms due to hyperprolactinemia, such as galactorrhea.
A third indication is in women with mild hyperprolactinemia and normal cycles who are trying to conceive as they may have subtle luteal phase dysfunction.