Wilson’s disease
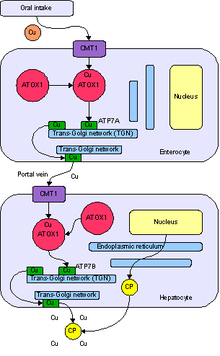
Mutation in the Wilson disease protein (ATP7B) gene, a protein transporting excess copper to bile.
Copper build-up in the brain and liver mostly, which can cause fulminant liver failure.
Other organs
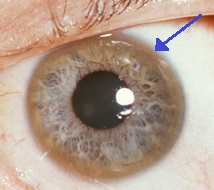
Eyes: Kayser-Fleischer rings
Kidney: RTA type 2
Heart: Cardiomyopathy
Hormones: Hypoparathyroidism
Diagnosis
- Serum and urine copper:
Urine copper Interpretation:
Normal dU copper (24 hr) ………………… 15-36 ug/24hr
Indicative of Wilson’s Disease …………… 40-100 ug/24hr
(Need to confirm with additional test)
Confirms Wilson’s Disease ……………….. >100 ug/24hr
Serum Copper will paradoxically be low. This is because ceruloplasmin (copper-binding protein) is low in 80-95% of patients with Wilson’s disease.
2. Ceruloplasmin low (remember it’s an acute phase protein)
3. Liver biopsy
4. Genetic sequencing of the ATP7B gene.
Treatment
Low Copper diet (avoid copper cutlery)
Penicillamine (Cuprimine – not available in South Africa) binds Cu by chelation and excretion in urine (but causes drug-induced lupus and Myastenia Gravis in 20%)
Trientine also chelates.
Zinc stimulates metallothionein, a protein in gut cells that binds copper and prevents their absorption and transport to the liver. As soon as urine Cu excretion is in normal limits, patients will go on to Zn therapy.
Asymptomatic pts. (by family gene screens) are treated, because copper accumulation will cause problems later. Usually Zn is used.
Images are all from Wikipedia
