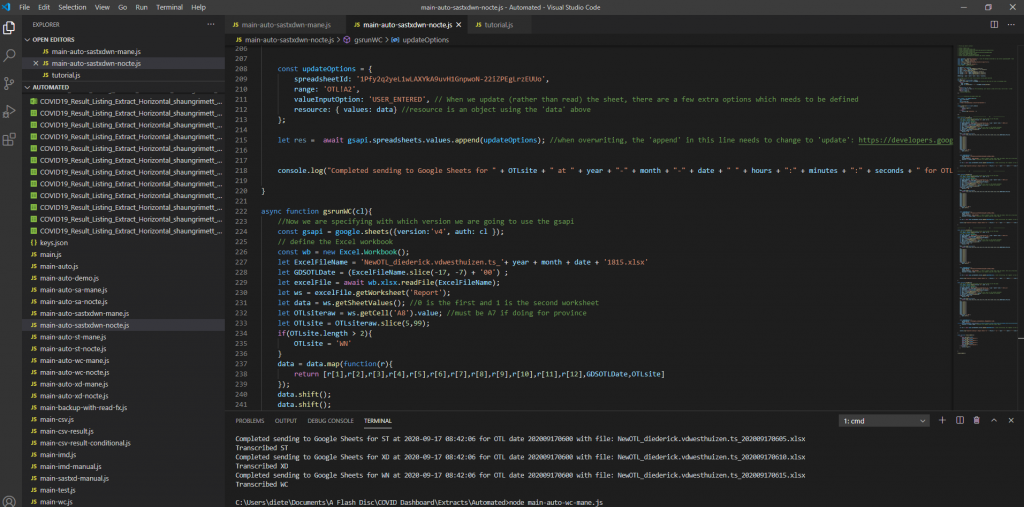
A dashboard was created to visually represent the COVID outstanding test list for our province for COVID outstanding PCR tests. This dashboard has been requested by the area manager of the Western Cape and various others on the Virology Expert Committee. Even though not a task primarily assigned to chemical pathologists, since I have an interest in data science, I tried to help. The end result was a dashboard which is updated every morning at 06h00 and every evening at 18h00 with a few JavaScript scripts running each day, updating three databases on the backend along with automated data extractions being done from TrakCare every morning and evening at a predefined time.
Screenshot 1 – Illustration of the JavaScript code to read the extracted Excel (or CSV) files and transcribing them to a Google Sheets database.
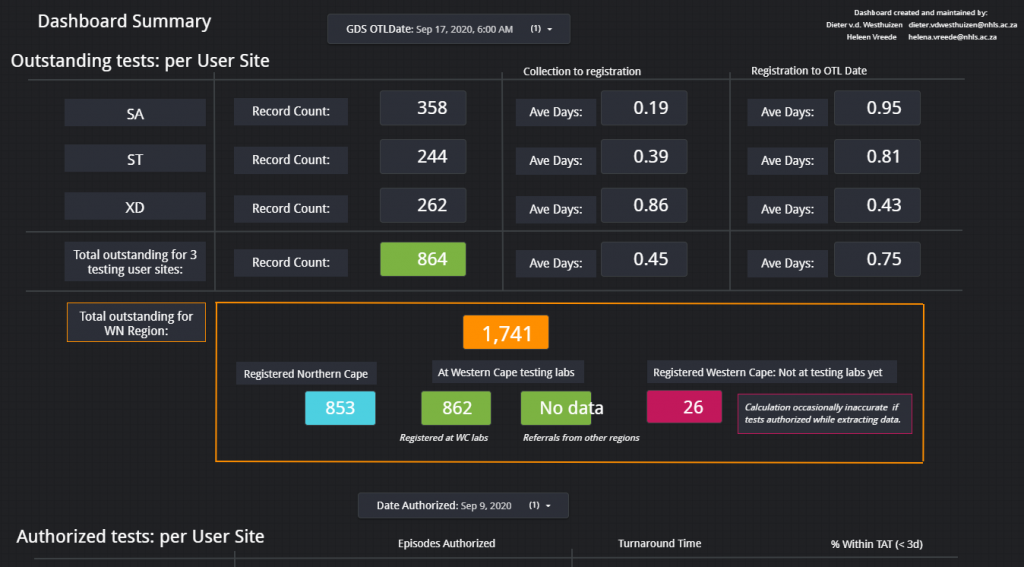
This dashboard was used (and likely still are being used) especially by the virologists at Groote Schuur Hospital to track the progress of outstanding COVID PCR tests and it can also be used to show possible bottlenecks in pre-analytical sample issues if tests are already registered before being sent to any of our laboratories in the Western Cape.
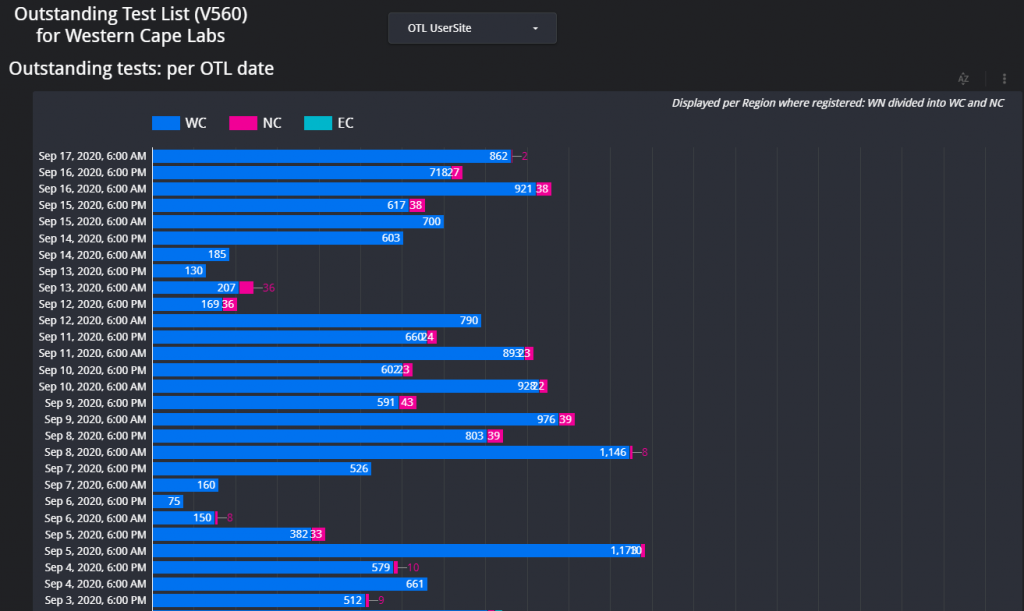
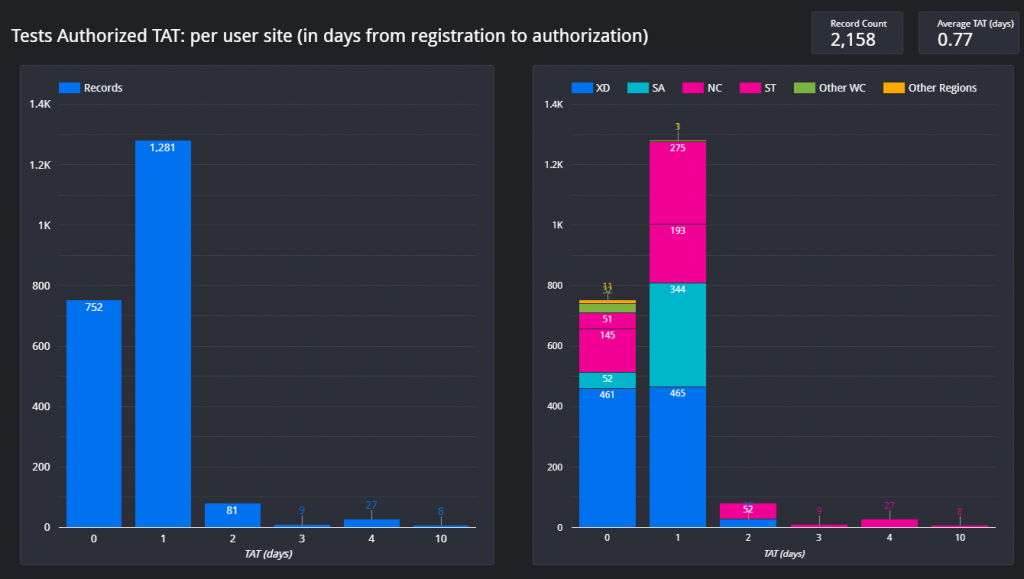
Figure 1 – Screenshot of the Dashboard. Follow the link above to view.Figure 2 – Example of the layout of the page which shows the total count of items on the respective outstanding test lists for each respective data for the Western Cape.Figure 3 – Outstanding tests summary by location. This page is especially helpful if the delay / outstanding tests from a specific hospital or clinic needs to be visualized in comparison with other locations (hospitals / clinics).Figure 4 – Illustration of the turnaround time met by a certain count of samples per each respective user site for one day.
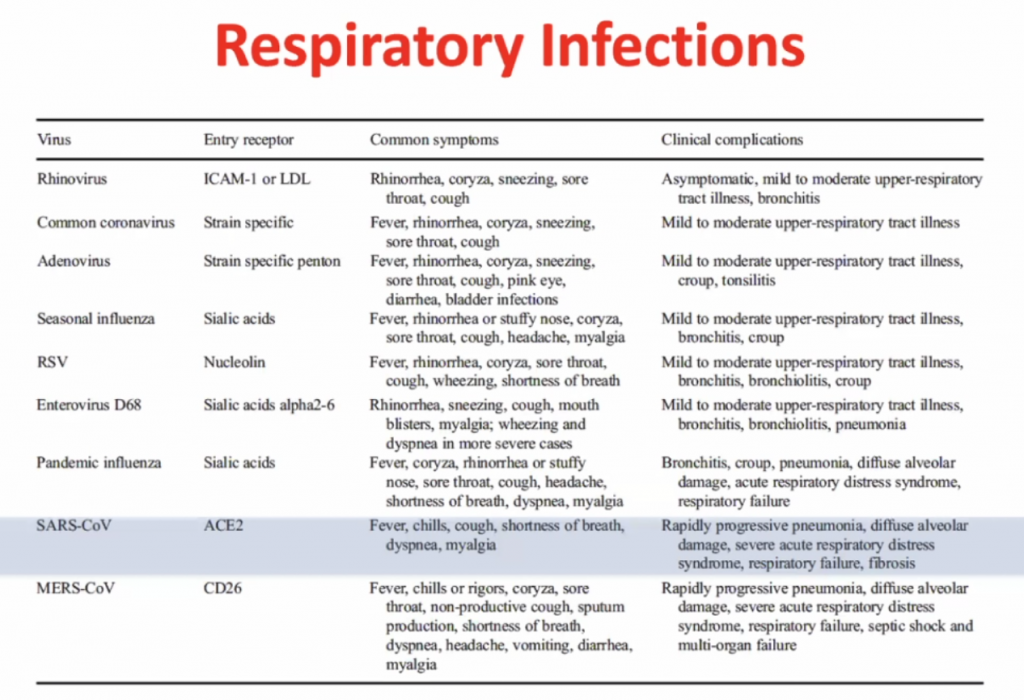
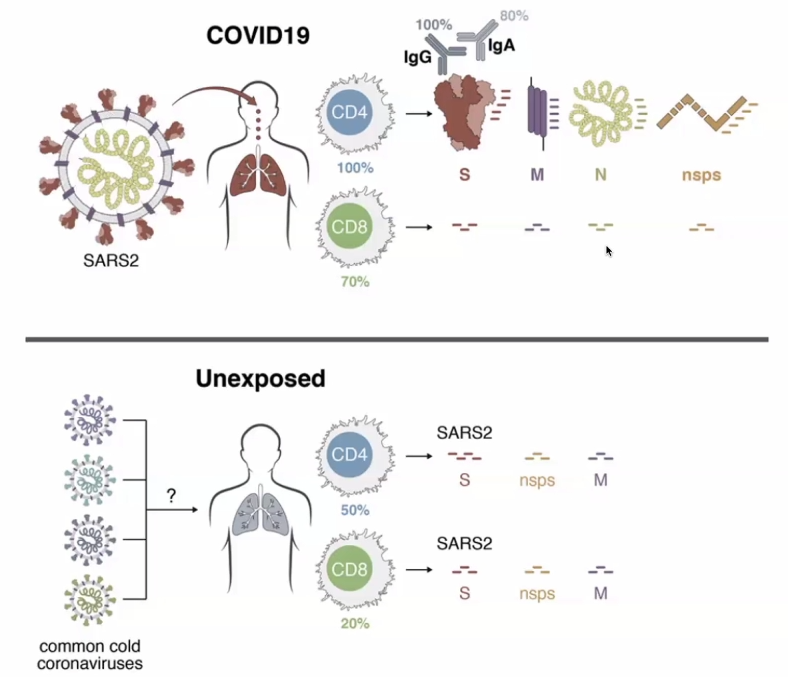
Immune Responses to SARS-CoV-2 cause severe COVID-19 in some and recovery in most
Clive Gray – Professor in Immunology immunopaedia.org – useful web site for immunology resources.
Outline:
Basics of Immunology
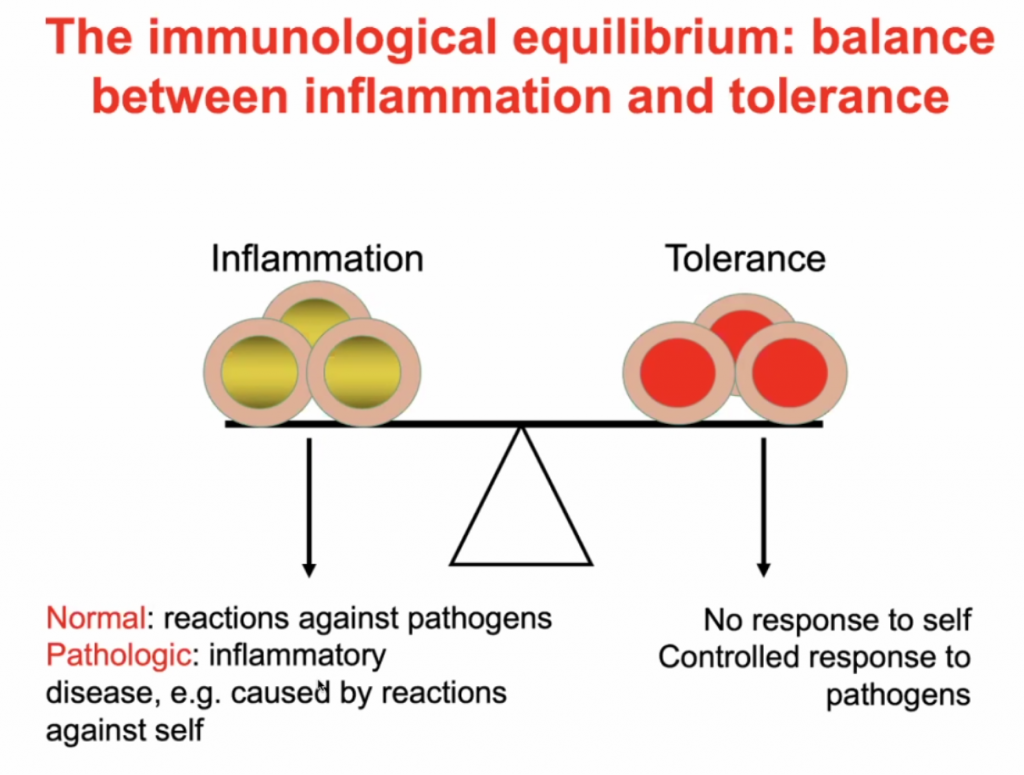
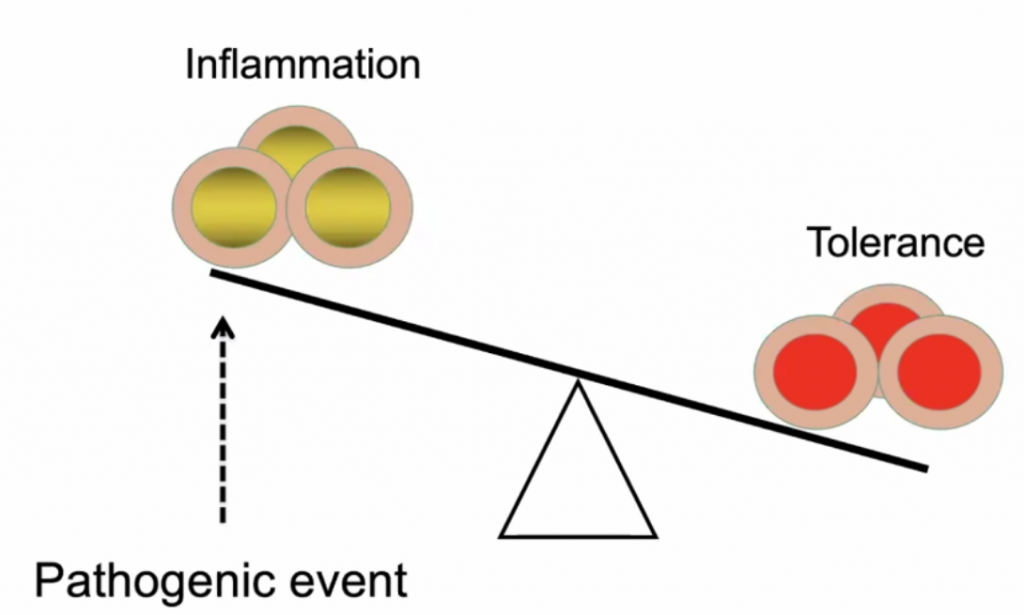
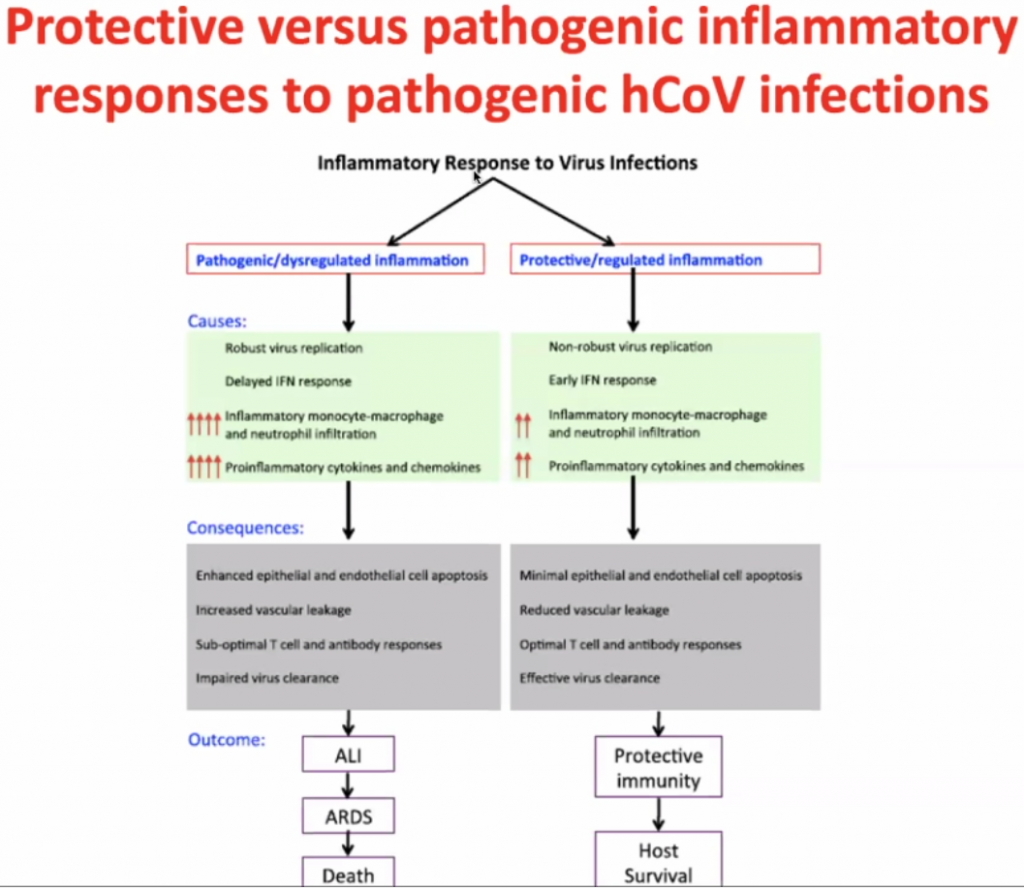
A balance between inflammation and tolerance
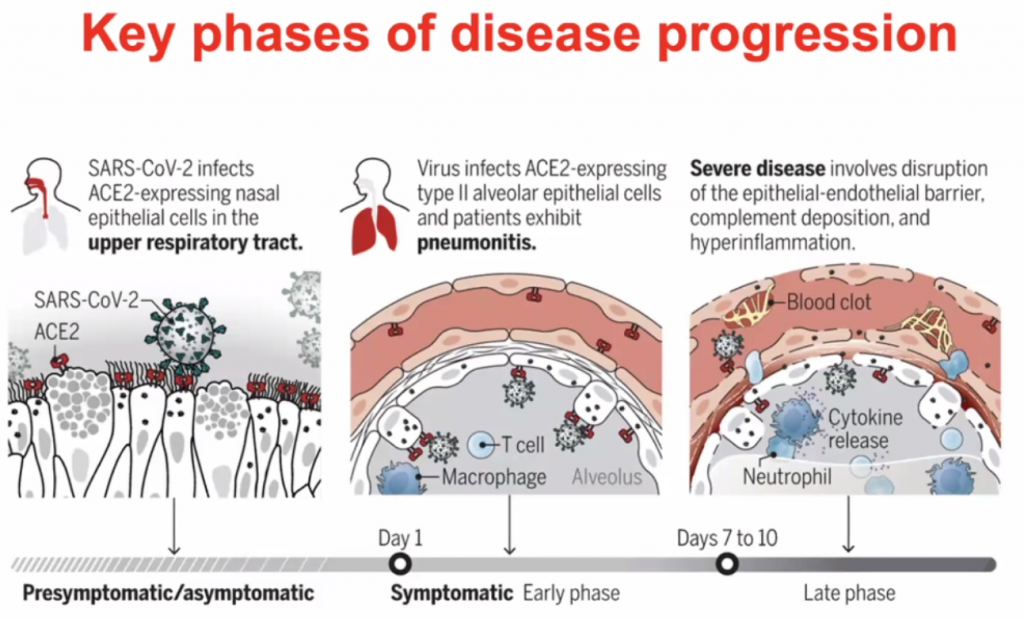
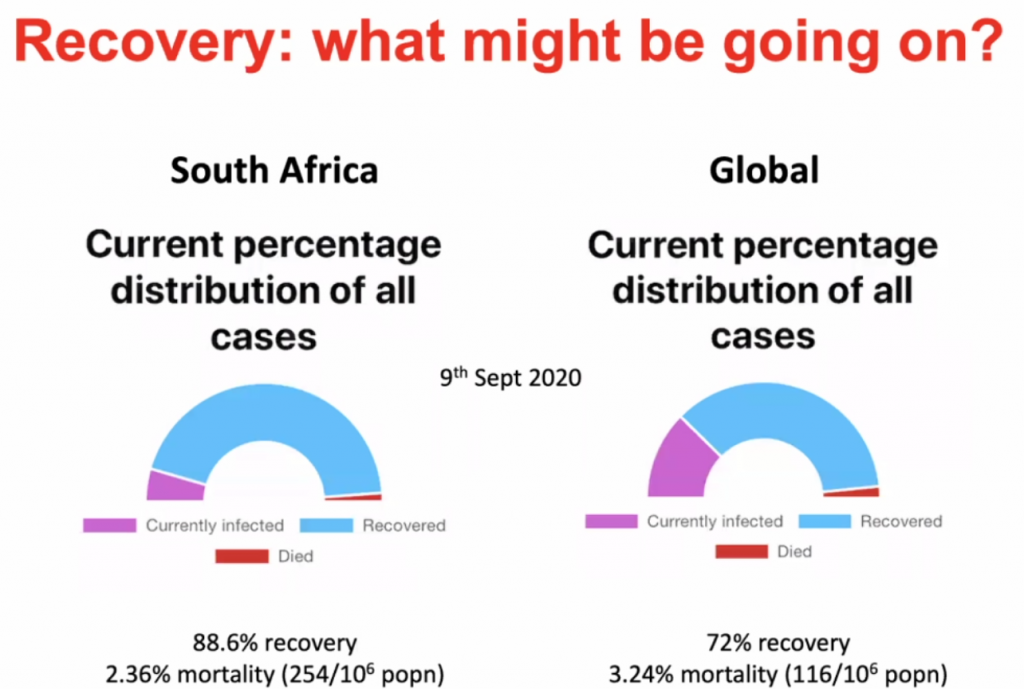
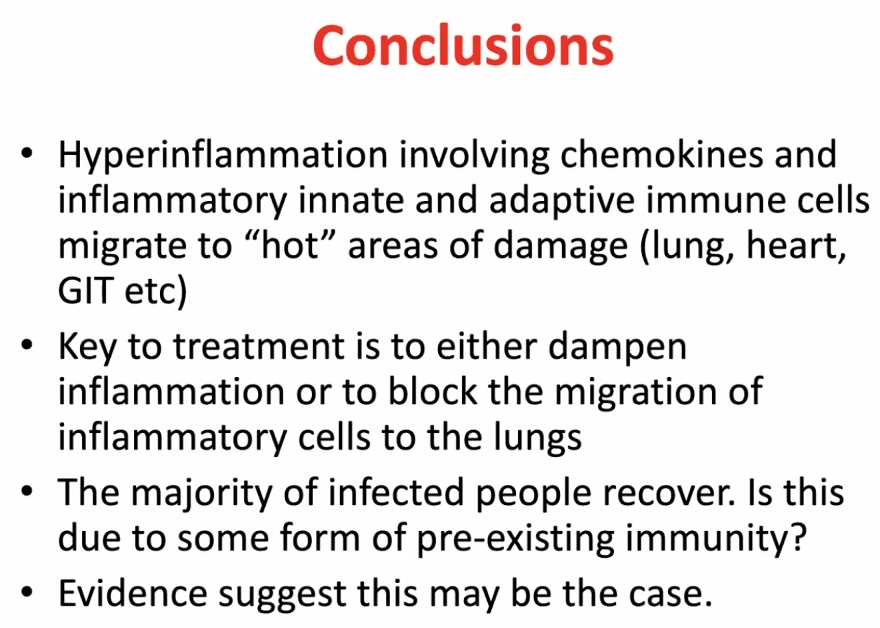
What happens to people who progress to severe COVID-19?
What might be happening in SARS-CoV-2 infected people who remain asymtomatic, have few symptoms and recover?
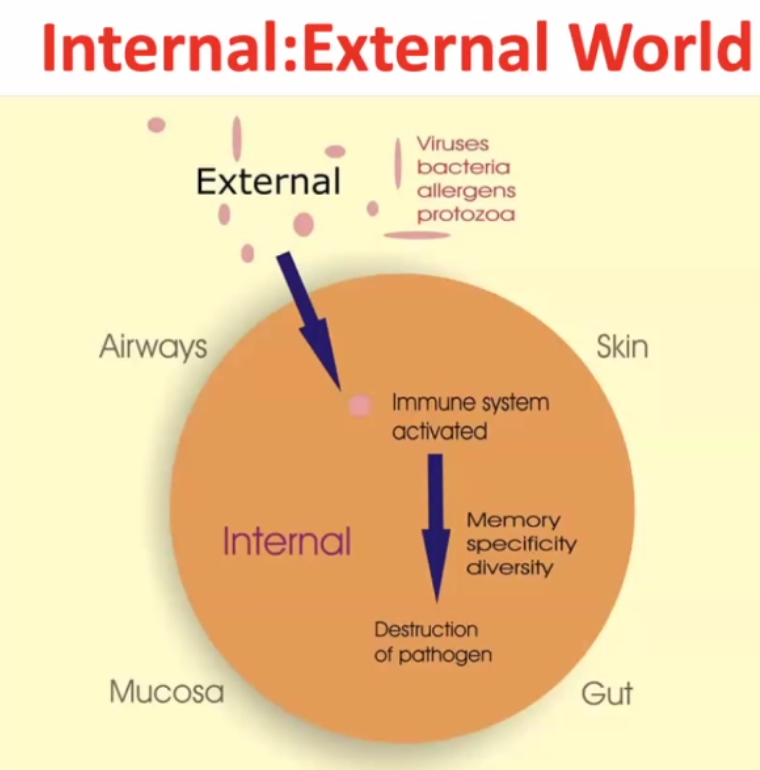
Internal : External world
~99% of time the pathogen gets destructed, but the pathogen may survive in rare cases.
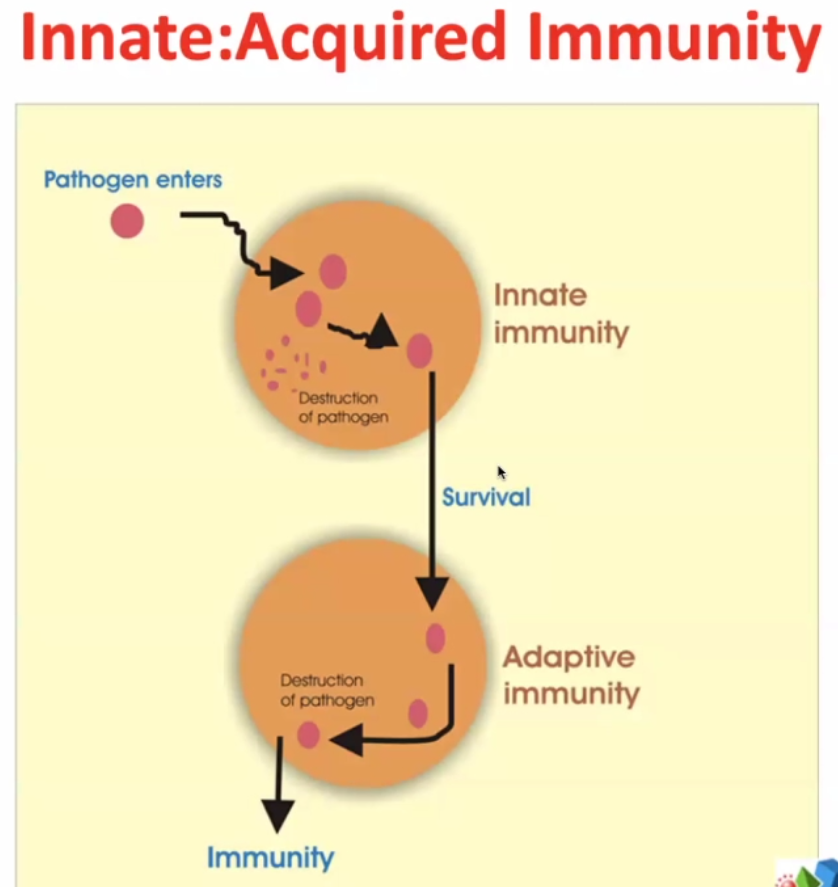
2 arms of immune responses:
Innate – evolutionary response – very rapid – elements of innate immunity are found in bacteria, plants, lower vertebrates, squids, fish etc.
Some pathogens survive ->
Adaptive immunity – much more targeted / focussed. The immune system targets more specifically the pathogens which survive the innate immunity.
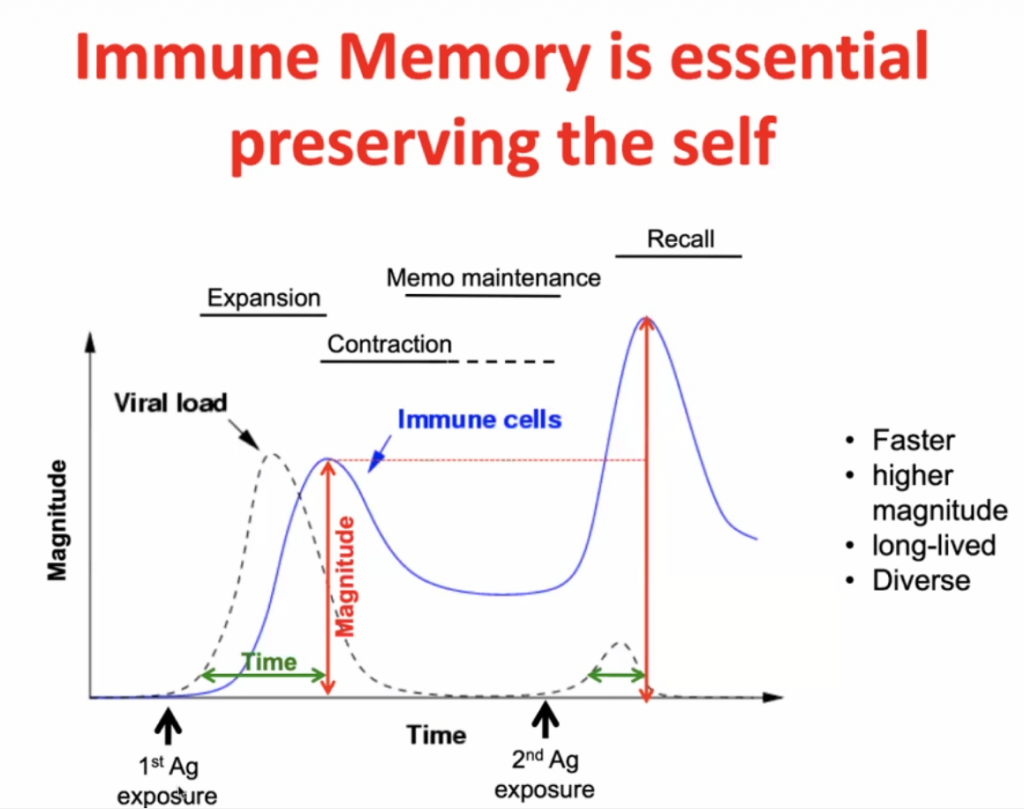
Infection initially -> expansion (peak after maximal viral load) -> contraction with some residual immunity (Memo Maintenance) -> with secondary response (Recall) there is a more rapid expansion (and higher peak) of the specific immunity.
Immune regulation:
Predisposed conditions: DM, HPT, Obesity, would make an individual highly susceptible to inflammation due to in imbalance of Inflammation vs. Tolerance, see below.
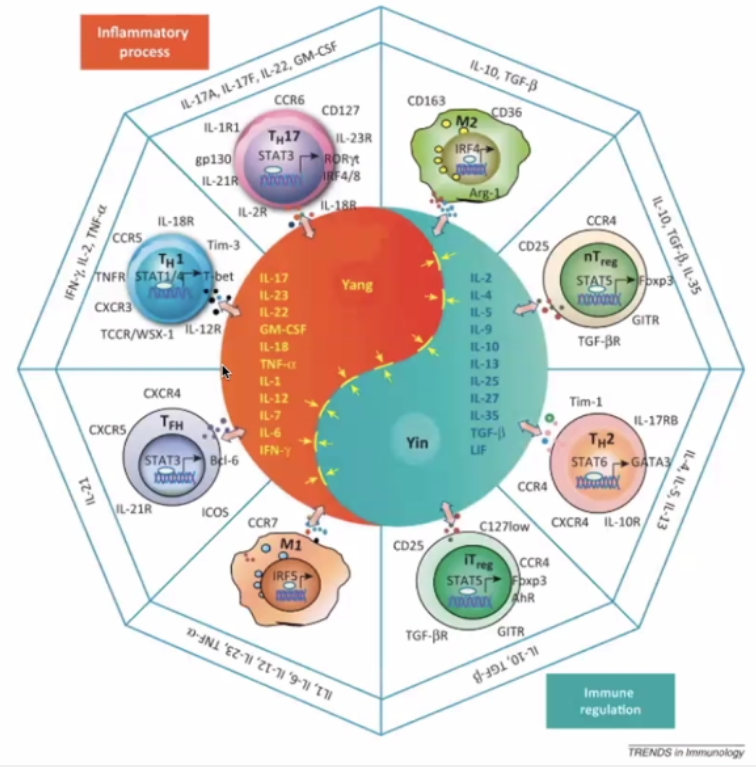
The Yin Yang of immunology:
Yin – immune regulation; Yang – Inflammatory Process
Pro-inflammatory (Orange)
TH17 – inflammatory cells secreting the “calling signals” for leucocytes.
Macrophage – presents antigens – in lymph nodes and germinal centres
T-Helper cells T-FH
Immune Regulation (Blue)
TH2 – hand in hand with TH1 (opposite)
Regulatory cells (nT and iT regulatory cells)
Actual pathogen is not causing disease – but the immune response – thus this is what should be focussed on to treat the disease.
Dose of the virus (viral load) is key to how you respond to the virus – Initial High dose in viral load likely will lead to high inflammatory response; Low dose (non-robust virus replication) may cause a less severe inflammatory response.
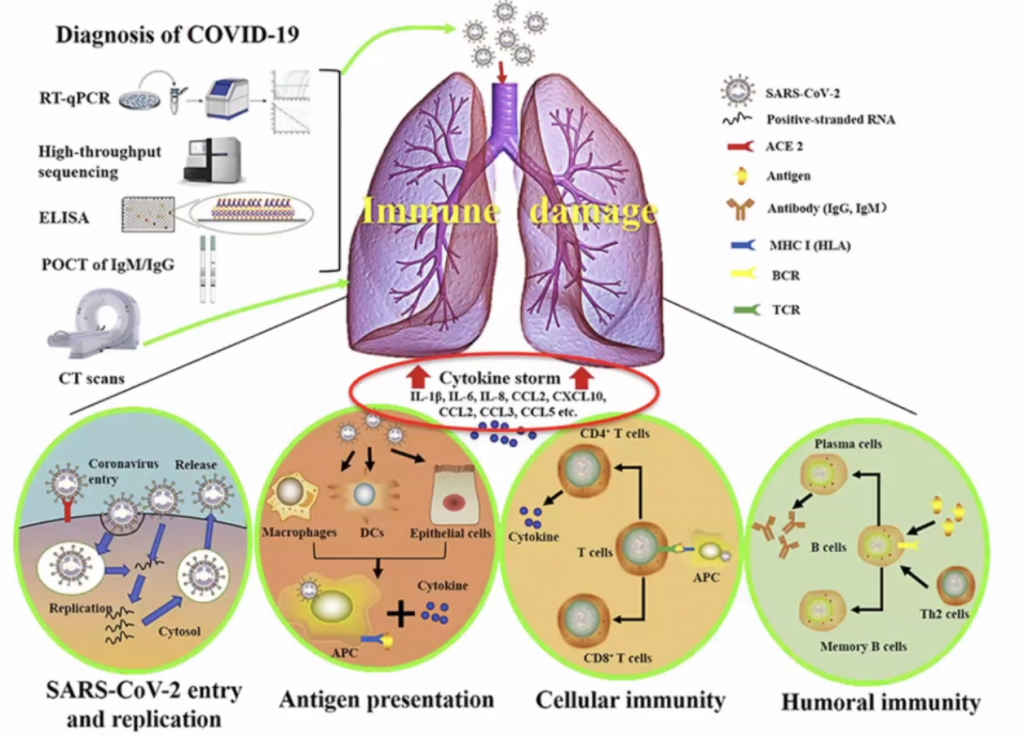
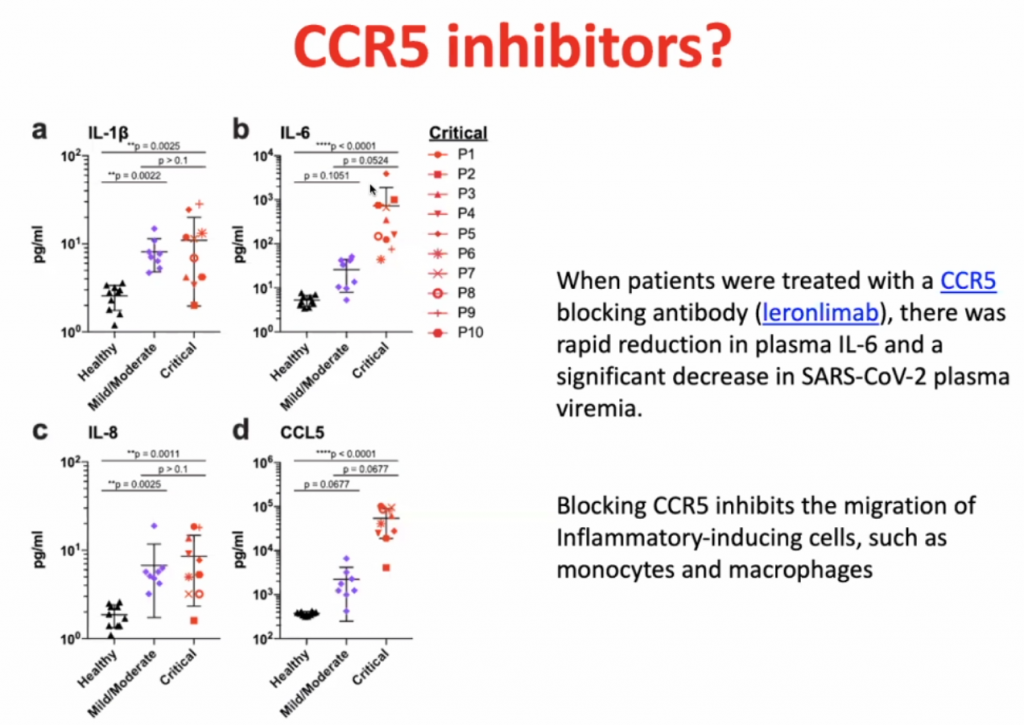
CCL’s allow leucocytes to migrate, hence in a cytokine storm, with high level of migration, the leucocytes causes severe local inflammation due to migration of leucocytes to local sites.
CCL5 blocking antibodies leads to rapid reduction of IL-6.
Dexamethasone is not so much an inhibitor of CCR5, but it prevents the hyperinflammation by inhibiting the majority of the inflammatory pathway.
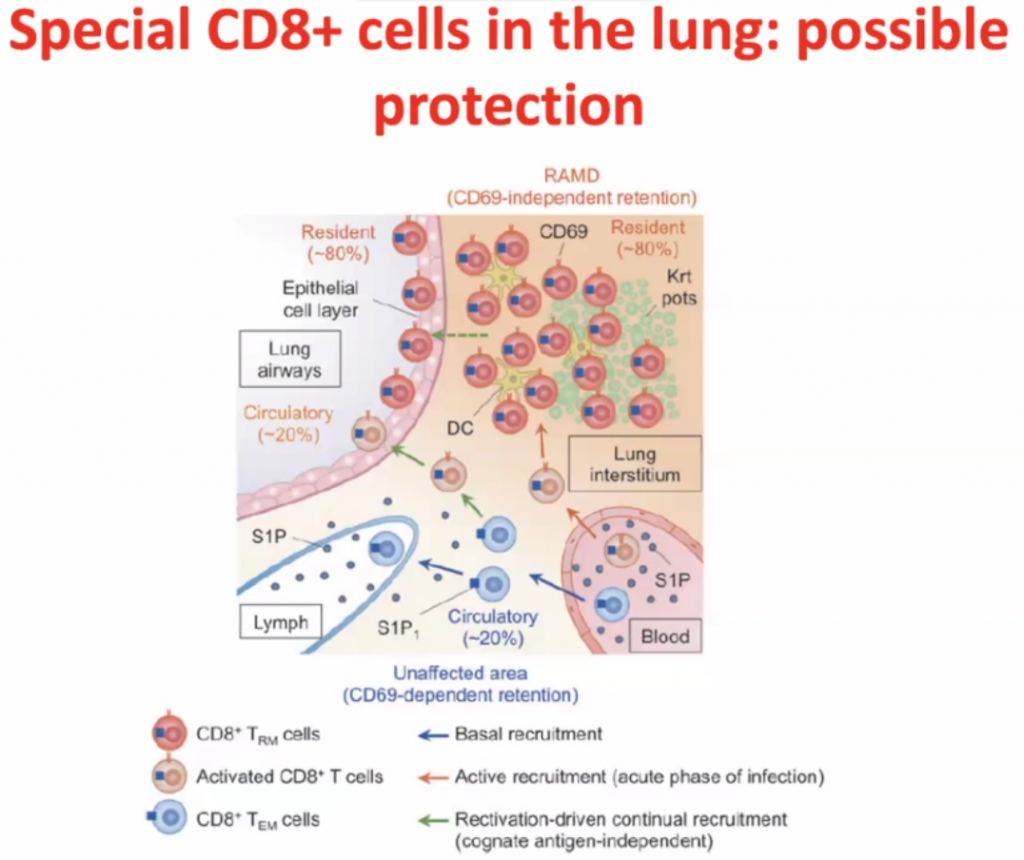
CD8 cells
Within interstisium, the CD8 cells are present and
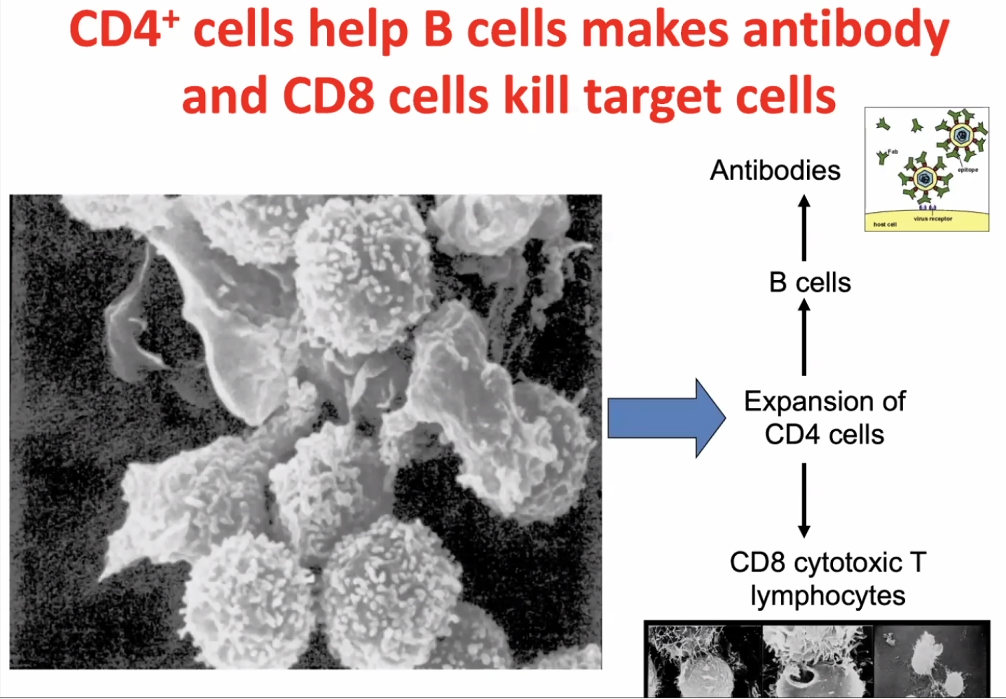
CD4 cells activates CD8 cells, hence called T-helper cells.
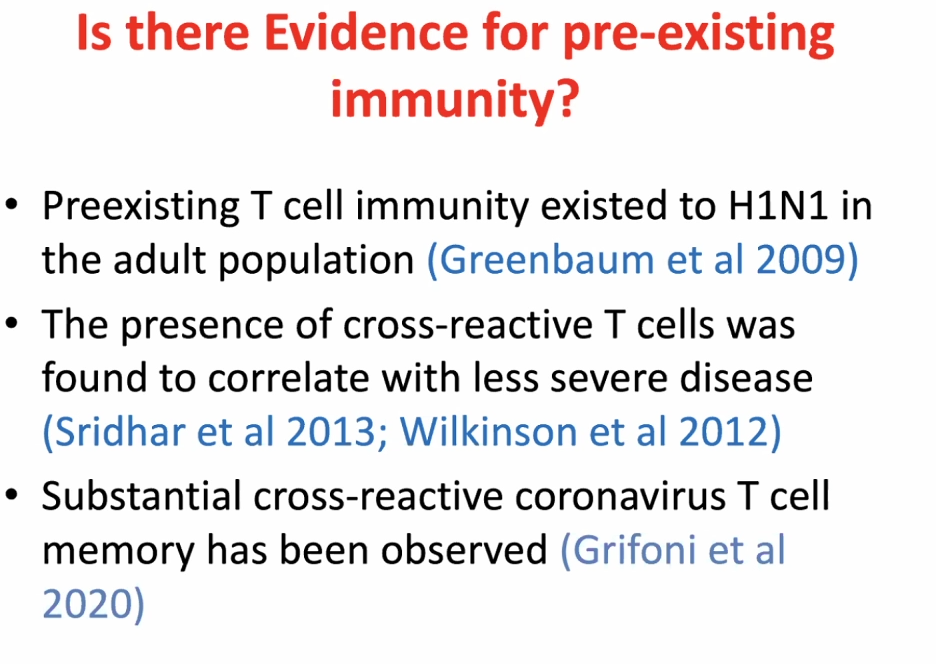
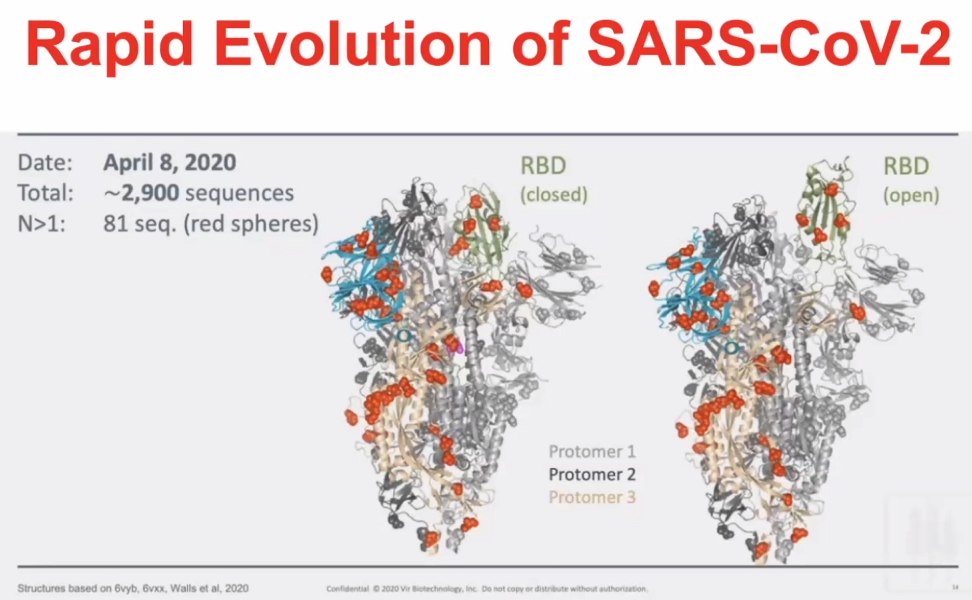
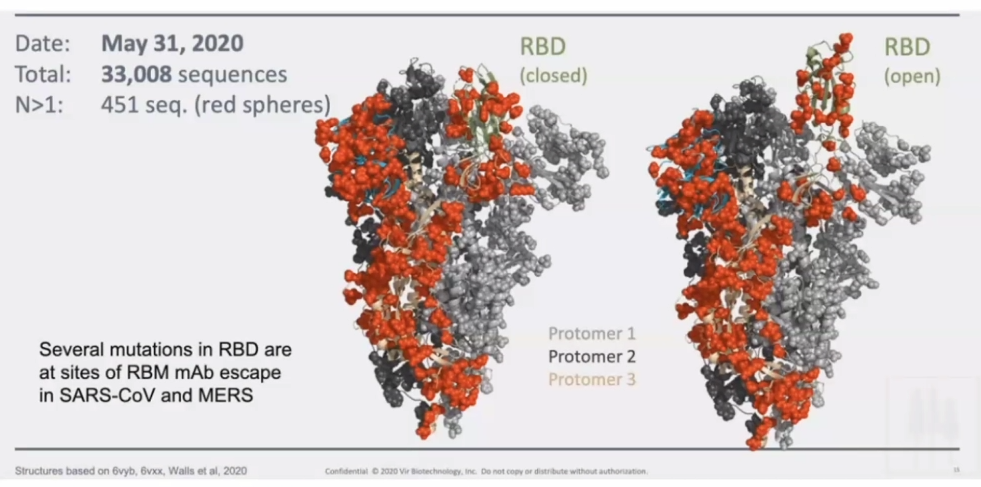
T-cell responses are very prevalent to COVID-19 exposed individuals. BUT CD4 cells and CD8 cells can also react to the SARS2 viral proteins in unexposed individuals.RBD – receptor binding domain (Spike-protein); Orange is the amount of amino acids which are changeable.Orange amino acids are those which are changeable – illustrating how the virus has mutated in a month.
Section 7.1 – Publications by Candidate
COVID-19 Related Laboratory Analyte Changes and the Relationship between SARS-CoV-2 and HIV, TB and HbA1c in South Africa
Reinhardt Hesse, Dieter van der Westhuizen, Jaya George
We conducted a retrospective analysis on data of all adults tested for SARS-CoV-2 across our laboratory network in South Africa over a 4-month period. Out of 842,197 tests 11.7% were positive and 88.3% negative. The prevalence of HIV was 6.25 and 6.31% in the SARS-CoV-2 positive and negative cohort respectively (p=0.444). However, the prevalence of HIV positive individuals in the critical cohort (9.15%) was higher than in the non-critical group (6.24%) (p=0.011). Active tuberculosis infection was approximately 50% less in SARS-CoV-2 positive than in negative individuals. The prevalence of uncontrolled diabetes was 3.4 times higher in SARS-CoV-2 positive cases, but was not higher in the critical vs. non-critical cases (p=0.612). The neutrophil-to-lymphocyte-ratio, coagulation markers, urea, cardiac, and liver related analytes were significantly elevated in the critical compared to non-critical cases. Platelet count and creatinine concentration did not differ significantly between the two groups. These findings do not support increased prevalence of HIV or tuberculosis in individuals with SARS-CoV-2 infection but do suggest an association of increased disease severity with HIV positive status. Uncontrolled diabetes was positively associated with a significantly higher prevalence of SARS-CoV-2 and our investigation into analyte changes associated with SARS-CoV-2 disease severity supported previous findings of raised inflammatory markers, coagulation markers, liver and cardiac related analytes and urea, but not for creatinine and platelet count.
Acute Kidney Injury during the COVID-19 Pandemic – Experience from Two Tertiary Centres in South Africa
Nina E. Diana, Ismail S. Kalla, Nicola Wearne, Sarah Kariv, Bianca Davidson, Jody Rusch, Zibya Barday, Abid M. Sheikh, Samantha Reiche, Farzahna Mohamed, Sara Saffer, Chandni Dayal, Jacqueline P. Venturas, Jarrod M. Zamparini, Dieter van der Westhuizen, Sean Wasserman, Nectarios Papavarnavas, Linda Boloko, Timothy de Wet, Graham Paget, Adam Mahomed, Sagren Naidoo and Erika S.W. Jones
Background: The first case of SARS-CoV-2 in South Africa [SA] was documented in March 2020. By October, the total cases for the Western Cape and Gauteng Provinces were 331,425 with 8456 fatalities. The aim of this study was to describe the prevalence of acute kidney injury [AKI] in hospitalized patients with COVID-19 in two tertiary centres in SA. Methods: SARS-CoV-2 positive patients admitted to two tertiary centres in SA between 18 March and 31 August 2020 were included in the study. Demographic data, pre-existing comorbidities, admission variables, laboratory data, management and hospital outcomes were captured. Exclusion criteria included age <18 years, pre-existing Stage 4 or 5 chronic kidney disease and prior renal transplant. Outcomes assessed were the need for acute dialysis, recovery from AKI, discharge and death. Results: AKI occurred in 374/1102 (33.9%) patients admitted to the two hospitals. Within the AKI cohort, 91 (24.3%) patients required intensive care unit [ICU] management, and 32 (8.6%) received kidney replacement therapy. Older age (P = 0.001), pre-existing hypertension [HPT] (P = <0.0001) and biochemical evidence of severe disease, including high ferritin, lactate dehydrogenase, d-dimer and C-reactive protein, were significantly higher in the patients with AKI versus those without. AKI Stage 3 had a higher mortality and lower rates of renal recovery upon discharge. AKI was significantly associated with an increased utilization of ICU resources, prolonged length of stay and mortality. Conclusion: This study reports the largest cohort of COVID-19-associated AKI in Africa. Older age, HPT and severe COVID-19 infection were significantly higher in patients with COVID-19 who developed AKI. This cohort had high rates of AKI which was associated with adverse outcomes, including mortality.