A case of Primary hyperparathyroidism and subsequent parathyroidectomy
| HOSP # | WARD | Medical Ward | |
| CONSULTANT | Dr. Jody Rusch | DOB/AGE | 59 Y Male |
Abnormal Result
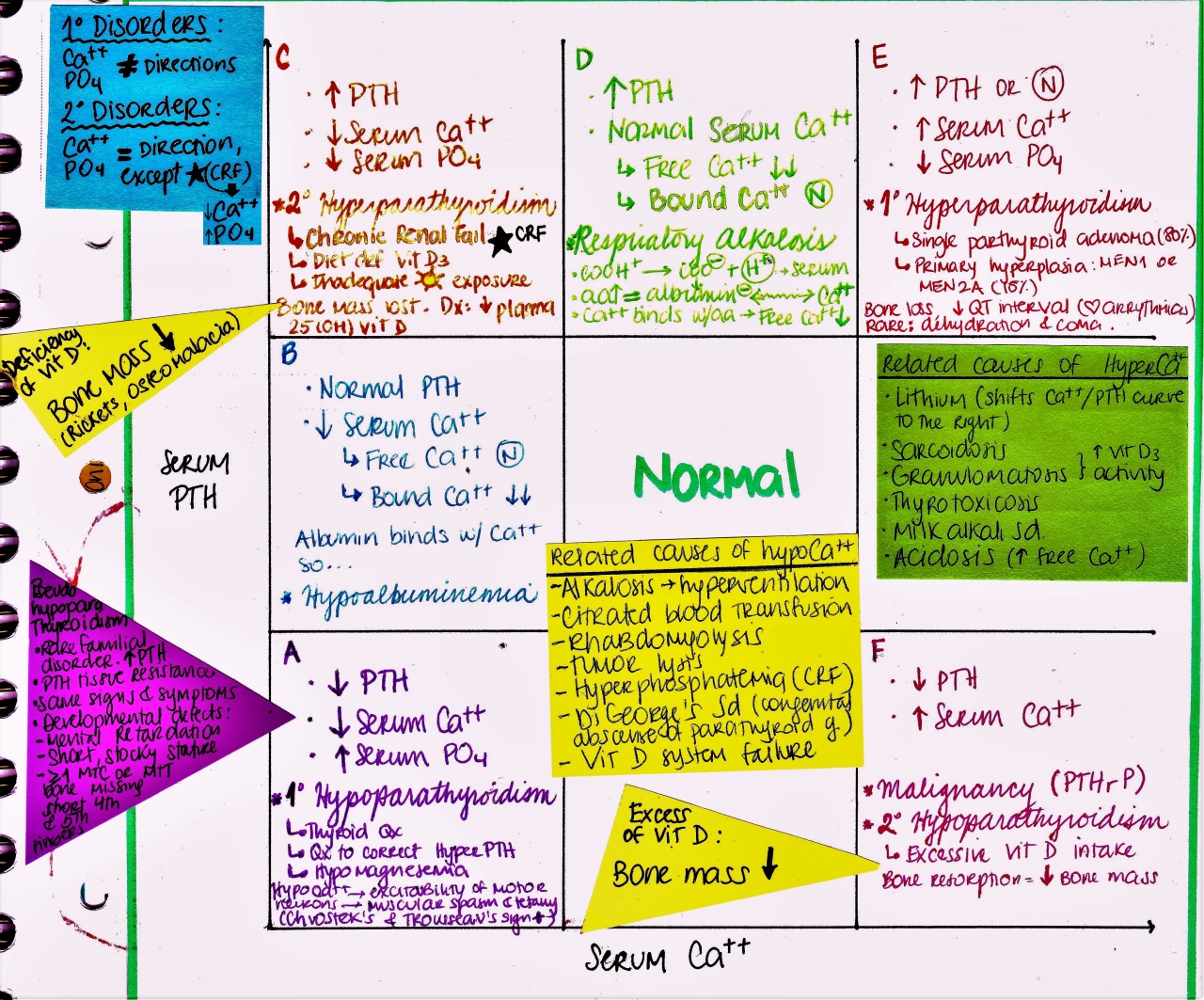
Hypercalcemia with hypophosphatemia
Presenting Complaint
History
This is a patient with parathyroid adenoma (and resulting longstanding hypercalcemia and hypophosphatemia, which is typical). Adenoma was removed yesterday, acc. to what I can see on a frozen section. Phosphate is dropping even more 0.42 mM (0.78 – 1.42) (on bloods taken this afternoon) and it will likely become significantly lower even.
Examination
Laboratory Investigations

PTH was initially significantly raised, although the renal function was normal. This means that there is likely hypercalcemia due to primary hyperparathyroidism.

Other Investigations
Final Diagnosis
Take Home Message
Phosphate supplementation may be quite important as there was longstanding autonomous PTH secretion, depleting stores of phosphate via phosphaturia (also PTH induced). There will likely not be much PTH secretion for some while, hence Vit. D activation will seize and little phosphate absorbed from the GIT due to longstanding lack of phosphate transporters. FGF-23 secretion will also seize and with the lack of PTH, the bone will not resorb and the remodeling process will consume the phosphate in the blood. Most mechanisms to increase phosphate physiologically will likely be dysfunctional at this time. Because he will not adequately absorb phosphate from the GIT (because of failure to activate Vit. D, he may need supplementation of phosphate IV).
Kidneys will however be a bit less phosphaturic (due to lack of PTH), thus he may respond quite well to IV phosphate.