Bilateral adrenal vein sampling
| HOSP # | Mr JB | WARD | Endocrine Department – CathLab – UCT private Hospital |
| CONSULTANT | Dr Jody Rusch | DOB/AGE | 53y Male |
Abnormal Result
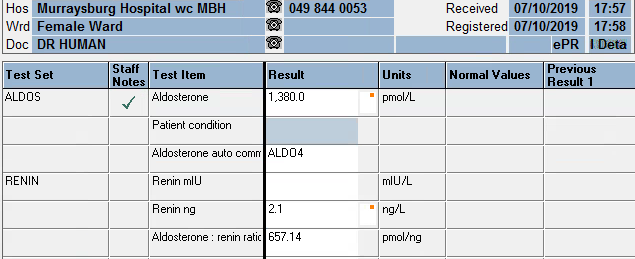
Upon authorizing blood results I came across a aldosterone result of 23300 pmol/L.
After a moment of brief anxiety, luckily I realized this was part of a series of tests performed by my colleagues in the Department.
Presenting Complaint
Medical complaint: Suspected Conn’s disease – right adrenal lesion/ irregular left adrenal gland.
History
The patient was confirmed to have primary hyperaldosteronism.
Unfortunately more information is not known. We were asked to assist with the sampling and the whole history weren’t available.
Examination
Not available
Laboratory Investigations

Other Investigations
Not available for this patient.
Ideally one would need a CT with contrast beforehand to adequately visualize the positions of the adrenal veins, as this may aid in the canulation, especially of the right adrenal vein.
One needs to diagnose hyperaldosteronism (by an appropriate salt loading test) before proceeding to bilateral adrenal vein sampling.
Final Diagnosis
Interpretation
| Definition | Formula | Clinical significance |
| Selectivity index | PCC(side) / PCC (ivc) | >cutoff confirms canulation of adrenal vein >3 stimulated >2 unstimulated |
| Lateralization index | PAC/PCC (dom) : PAC/PCC (non-dom) | >cutoff confirms laterilization of hyperaldo secretion >4 stimulated >2 unstimulated |
| Contralateral suppression index (used if inadequate canulation) |
PAC/PCC (non-dom) : PAC/PCC (ivc) | <cutoff (<1 or <0.5 – sources differ) indicate ipsilateral suppression and suggest contralateral aldosterone overproduction. |
PCC: plasma cortisol concentration, PAC: plasma aldosterone concentration, ivc: inferior vena cava or peripheral vein, dom: dominant side, non-dom: non-dominant side.
Selectivity index
Right: 1.0 (mean)
Left: 19.0 (mean)
These two results indicate that the left adrenal has been canulated adequately, but the right vein inadequately.
Lateralization index
Unable to comment because of the inadequate canulation of the right adrenal vein. If determined, it would very likely provide a false result.
Contralateral suppression index
1.5 : 1.8 = 0.8
This falls in between some of the referenced cutoffs (<1 and <0.5)
All of the other samples also fall somewhere in this range. Biochemically, these results suggests inadequate right sided venous sampling (a commonly described problem)
Take Home Message
- Procedure is done in the Cath Lab
- The patient received continuous synacthen infusion – as this improves the sensitivity (or perhaps rather specificity) of the test.
- Done under imaging with contrast used for the localisation of the adrenal gland and adrenal vein
- Sequential sampling technique used, generally > 20 mins infusion
- Multi-disciplinary: nurses, anaesthetist, radiographer, intervention radiologists, students, chemical pathologists
- Difficulty with sampling right side for both patients
- Difficulty with interpreting results – most likely due to inadequate canulation of the right adrenal vein
Some important learning points
- Adrenal vein sampling may be a valuable tool that is underutilised
- Careful selection of patients essential – also patient should consent to surgical removal of the affected adrenal before this invasive procedure is initiated
- Inter-disciplinary approach is necessary
- Obtaining cosyntroponin (aka synacthen) can be difficult (Section 21), but recommended.
- Right adrenal access difficult: may require specific imaging. Recommended to start on the right or do simulataneous sampling.
- Adrenalectomy may be curative or help achieve better control of BP thus decrease associated morbidity and mortality in those with unilateral adenoma