A case of high HDL-cholesterol
| HOSP # | WARD | GP Clinic | |
| CONSULTANT | John Stanfliet / Jody Rusch | DOB/AGE | 73 year Female |
Abnormal Result
Abnormal lipid profile (see below)
Presenting Complaint
A 73 year old female was investigated with a full lipid profile after presenting with an increased total cholesterol upon routine screening at her general practitioner.
History
The patient had an increased Total Cholesterol, but was otherwise not unwell. Medication history unfortunately not available.
Examination
Not available
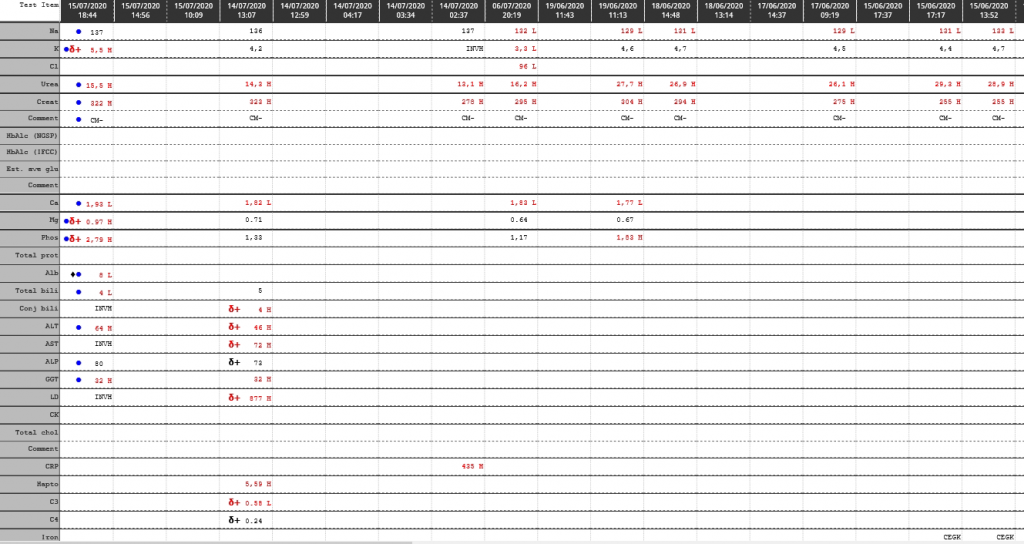
Laboratory Investigations
| Test | Result |
| Urea | 7.2 mmol/L |
| Creatinine | 105 umol/L |
| eGFR | 46 ml/min/1.73m2 |
| Fasting Lipid profile (lipemia index -turbidity- on sample was absent): | |
| Total Cholesterol | 6.7 mmol/L |
| Triglyceride | 0.6 mmol/L |
| HDL Cholesterol | > 4.7 mmol/L |
| Non-HDL Cholesterol (calculated) | < 2.0 mmol/L |
| LDL Cholesterol (calculated) | < 1.7 mmol/L |
| LDL Cholesterol (direct – measured) | 1.3 mmol/L |
| Glucose Fasting | 5.5 mmol/L |
Other Investigations
To rule out the possibility of interferents, the following tests were performed.
| Test | Value |
| Apo A1 | 4.24 g/L (424 mg/dL) (Ref. >140 mg/dL) |
| Apo B | 0.52 g/L (52 mg/dL) (Ref. < 130 mg/dL) |
| Apo B : Apo A1 ratio (calculated) | 0.12 |
Final Diagnosis
Increased HDL which may likely be an APOC3 deficiency.
Take Home Message
Although not present in this case, elevated apolipoprotein B (ApoB) confers increased risk of atherosclerotic cardiovascular disease, even in a context of acceptable LDL cholesterol concentrations. Extremely low values of ApoB (<48 mg/dL) are usually related to malabsorption of food lipids and can lead to polyneuropathy. Reduced apolipoprotein A1 (ApoA1) confers an increased risk of coronary artery disease. Extremely low ApoA1 (<20 mg/dL) is suggestive of liver disease or a genetic disorder. Elevated ApoB:ApoA1 ratio confers increased risk of atherosclerotic cardiovascular disease, independently of LDL and HDL cholesterol concentrations.
If the inverse of the above is true, then this lady is likely destined to live forever, but that’s the whole conundrum in lipid metabolism – the inverse of one’s theories does not always hold true under randomized controlled studies, and due to the difficulty of finding a proper control group. It was however previously demonstrated that patients with ApoC3 deficiency (if this is the cause in this case) increases longevity.
APOC3 has been established as an inhibitor for lipoprotein lipase, a gene that hydrolyzes triglycerides to generate free fatty acids before their uptake by muscle and adipose tissue (reviewed in Jong et al). Mice with a high-level expression of human APOC3 on a background of Ldlr deficiency proved to be an excellent model for familial combined hyperlipidemia, because they are disturbed in the breakdown of triglycerides. In contrast, mice lacking Apoc3 show increased activity of LPL, which causes hypotriglyceridemia and protection from postprandial hypertriglyceridemia. From these mice studies, it became clear that a deficiency of APOC3 could cause a healthier lipoprotein profile, which is associated with protection from cardiovascular diseases. However, in the absence of APOC3-deficient subjects, this hypothesis was difficult to test directly.
Dodacki, A., Wortman, M., Saubaméa, B. et al. Expression and function of Abcg4 in the mouse blood-brain barrier: role in restricting the brain entry of amyloid-β peptide. Sci Rep 7, 13393 (2017). https://doi.org/10.1038/s41598-017-13750-0