Quadruple-H
| HOSP # | 42170712 | WARD | Endocrinology OPD |
| CONSULTANT | Dr. Heleen Vreede | DOB/AGE | 37y female |
Abnormal Result
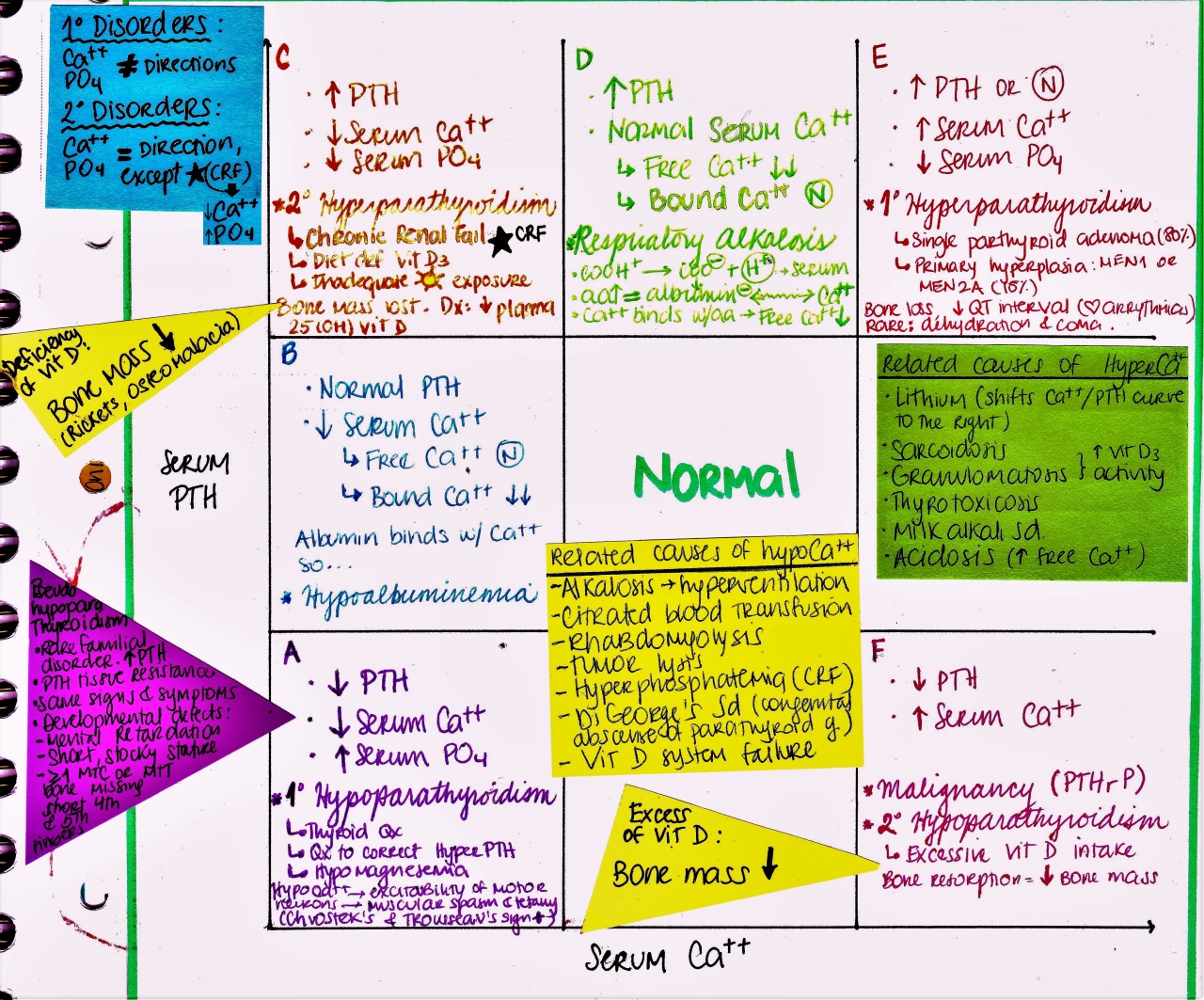
- The patient’s calcium measured 2.91 mmol/L on two occasions, with PTH measuring 40.6 pmol/L
- VitD 13.6 (<50 = deficient)
- TFT’s TSH 0.01 T4 26.7pmol/L
Presenting Complaint
Presented at the GIT clinic in Feb 2020 with persistent vomiting and abdominal cramps, which was ongoing since November 2019.
History
- Patient was diagnosed with hypertension in her early 20’s.
- Initiated on HCTZ – subsequently changed to Atenolol 25mg dly – not overweight at the time
- Gastroscopy was normal
- No psychiatric symptoms reported – mood swings are reported occasionally by the family
- Oligomenorrhoea – started in 2019 – nothing else wrong was noted.
- Normal menarche – normal regular menses until the diagnosis of hypertension was made.
- Amenorrhoeic last 4 years on no medication currently
Examination
- Increased BMI – quite significantly increased
- BP 170/90
- Skin: Significant amount of skin tags, acanthosis nigricans
- No striae or bruising
- No Sx of thyroid disease.
- Physical examination unremarkable.
- Normal pulses
- Essentially a normal examination other than the high BMI
Laboratory Investigations
Repeated bloods (5 days after initial presentation):
- TSH 3.13 T4 12.5
- PTH 28 pmol/L (1.6 -6.9)
- Ca 2.79
- Inorganic phosphate 0.77 L mmol/L (0.78 – 1.42)
- LFT’s: Normal
- Creat Normal
- U-Ca 5.6 (no creatinine to compare ratio)
- FSH 3.2 IU/L
- LH 2.0 IU/L
- E2 244 pmol/L
- Dehydroepiandrosterone sulphate (DHEAS) 2.4 umol/L (1.7 – 9.2)
- Testosterone 0.5 nmol/L (0.3 – 1.7)
- SHBG 25.9 L nmol/L (32.4 – 128.0)
- Prolactin 11.5
- TSH-Receptor antibodies: Negative
Other Investigations
The patient still had occasional vomiting, abdominal cramps and unexplained muscle pain – other electrolytes apart from calcium, magnesium and phosphate is also advised, as is osmolarity as fluid and electrolyte imbalance may be an effect, rather than a cause of the nausea, vomiting and muscle pain – the sodium and potassium was normal however.
See below, for the hypertension, phaeochromocytoma can be excluded by a 24-hour fractionated urinary metanephrines analysis.
Final Diagnosis
- Primary hyperparathyroidism is on top of the differential diagnosis and is likely the cause of the raised total calcium.
- Another cause of the raised blood pressure could very likely be a phaeochromocytoma.
- It was also advised for replacement of Vitamin D, after a repeat measurement.
- Other features of MEN-1 syndrome needs to be excluded.
Take Home Message
For phaeochromocytoma, 3 separate days’ urine collection is recommended if the suspicion is high, which it isn’t in this case. This increases the sensitivity of the test.
Before testing for MEN-1: one needs to correct Calcium first – since the hypercalcemia could exacerbate gastrin levels.
Increased serum calcium and hypophosphatemia is the net-result of increased PTH. Urinary phosphate will also be high if measured.