A case of Cryptococcal meningitis with hypomagnesemia
| HOSP # | WARD | Victoria Hospital Female medical ward |
|
| CONSULTANT | Heleen Vreede | DOB/AGE | 29y female |
Abnormal Result
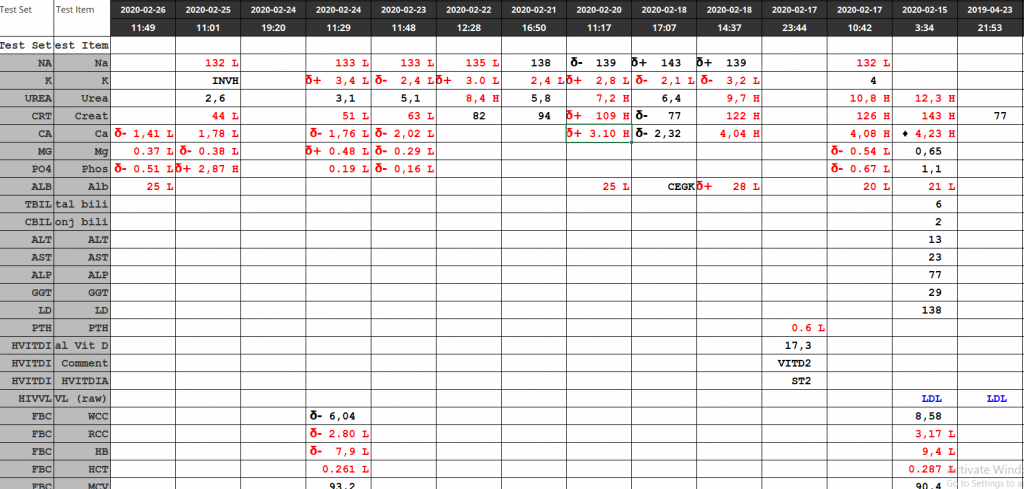
The magnesium result measured 0.36 mmol/L ( 0.63 – 1.05 mmol/L) despite adequate levels prior to admission to hospital (0.75 mmol/L on 18/04/2020).
Presenting Complaint
The patient was asymptomatic with regards to the at the time when the result was obtained.
History
Patient was diagnosed with Cryptococcal Meningitis on 22/04/2020 with a cryptococcal latex agglutination test.
Patient was known HIV positive with a CD4-count of 9 cells/uL (332-1642).
Examination
Unfortunately this data is not available.
The clinical features of hypomagnesemia is predominantly related to the derangement in the calcium becoming deranged when hypomagnesemia occurs.
Laboratory Investigations

Other Investigations
None available.
Final Diagnosis
Hypomagnesemia with accompanying hypocalcemia due to Amphoterecin B therapy
Take Home Message
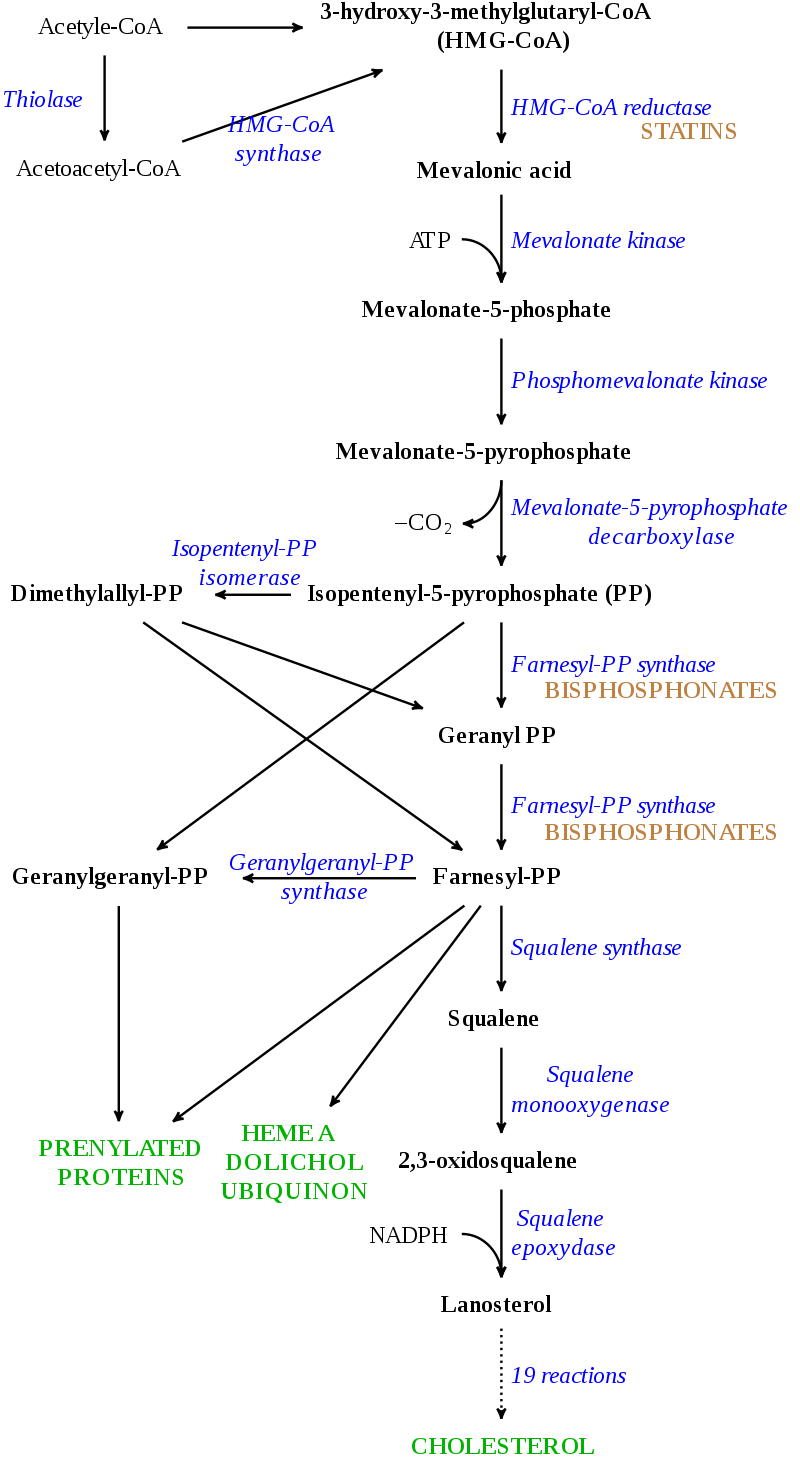
- I’ve learned from the attending clinician (and a short literature search) that Hypomagnesemia is a known consequence of Amphotericin B therapy.
- Hypocalcemia is often a consequence of hypomagnesemia (as in this case). This is due to two known mechanisms:
- Decreased sensitivity of Calcium at the calcium-sensing receptor, with decreased secretion of PTH and hence its effects.
- Decreased action of PTH due to PTH-receptor resistance being caused by hypomagnesemia.