Immune Responses to SARS-CoV-2 cause severe COVID-19 in some and recovery in most
Clive Gray – Professor in Immunology
immunopaedia.org – useful web site for immunology resources.
Outline:
- Basics of Immunology
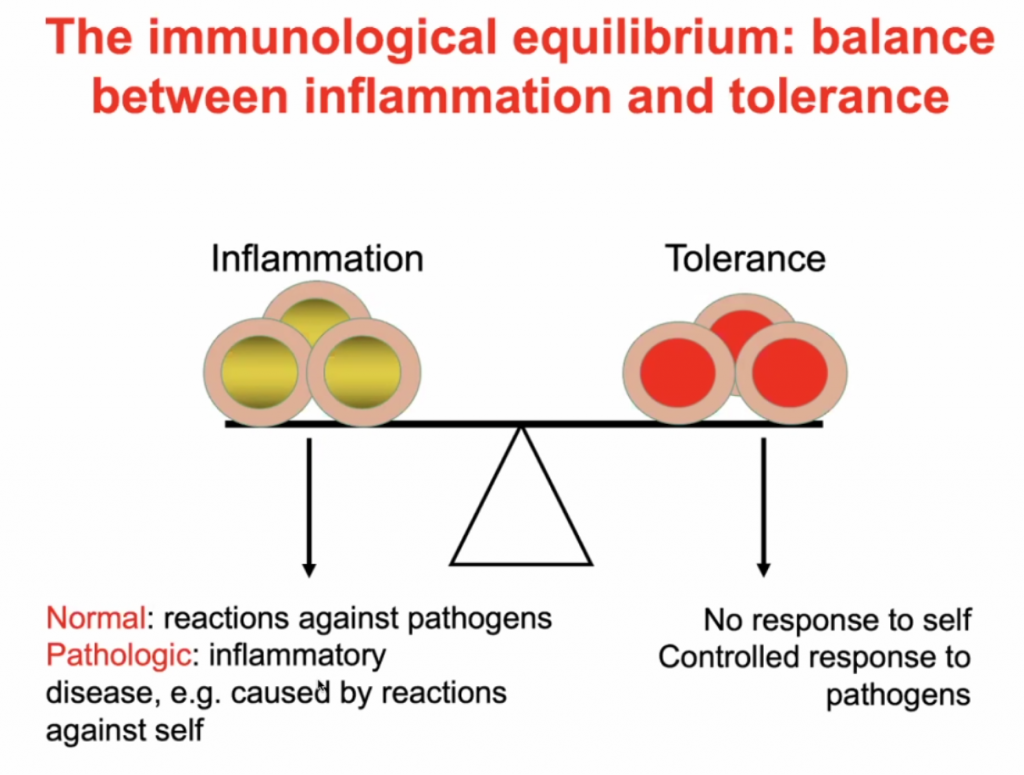
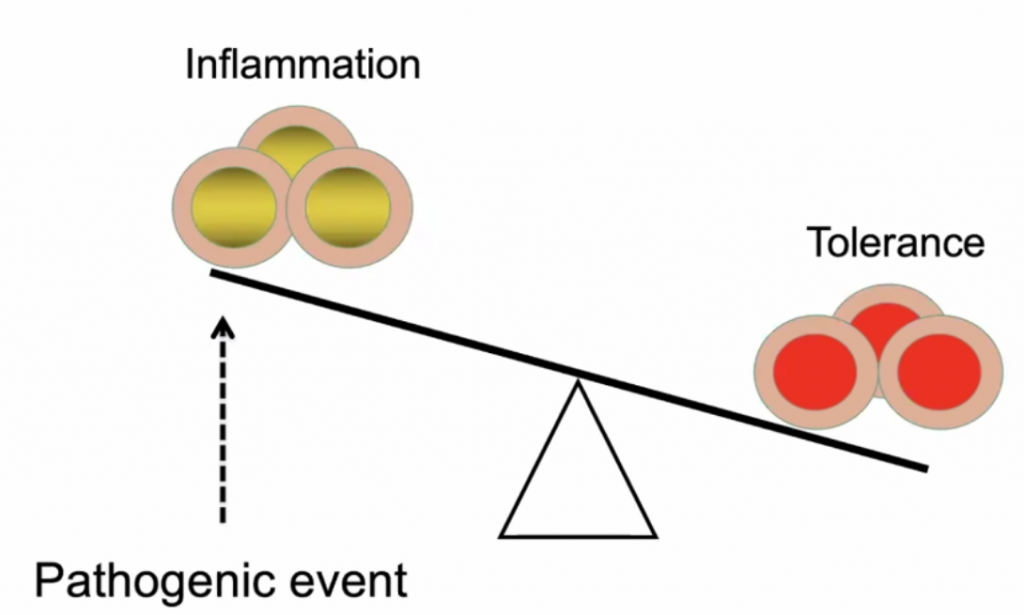
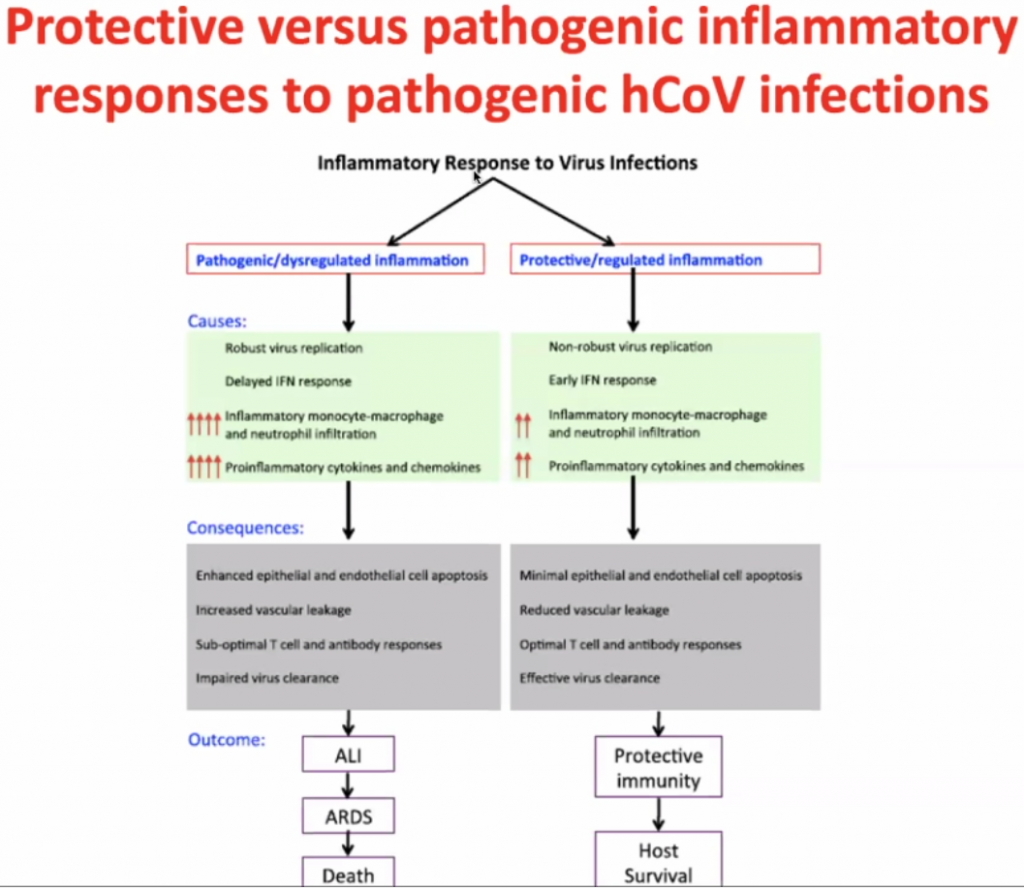
- A balance between inflammation and tolerance
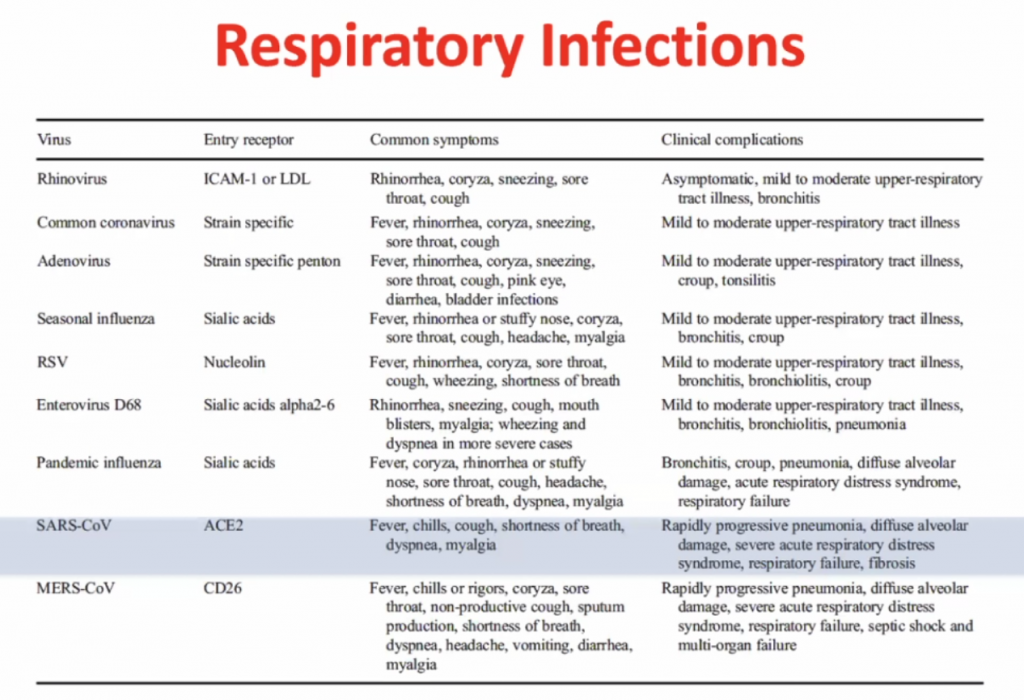
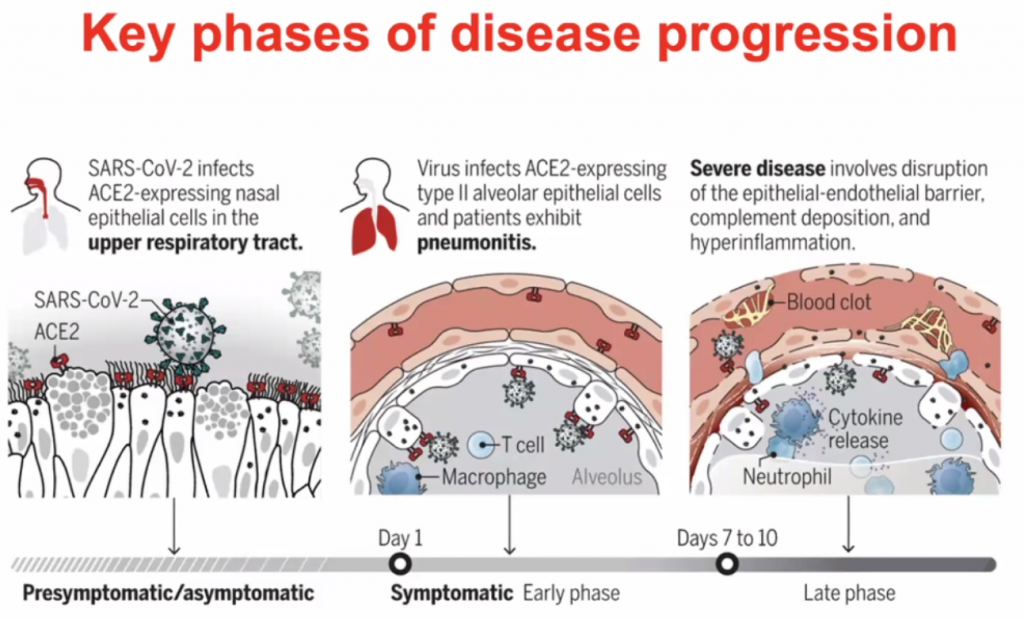
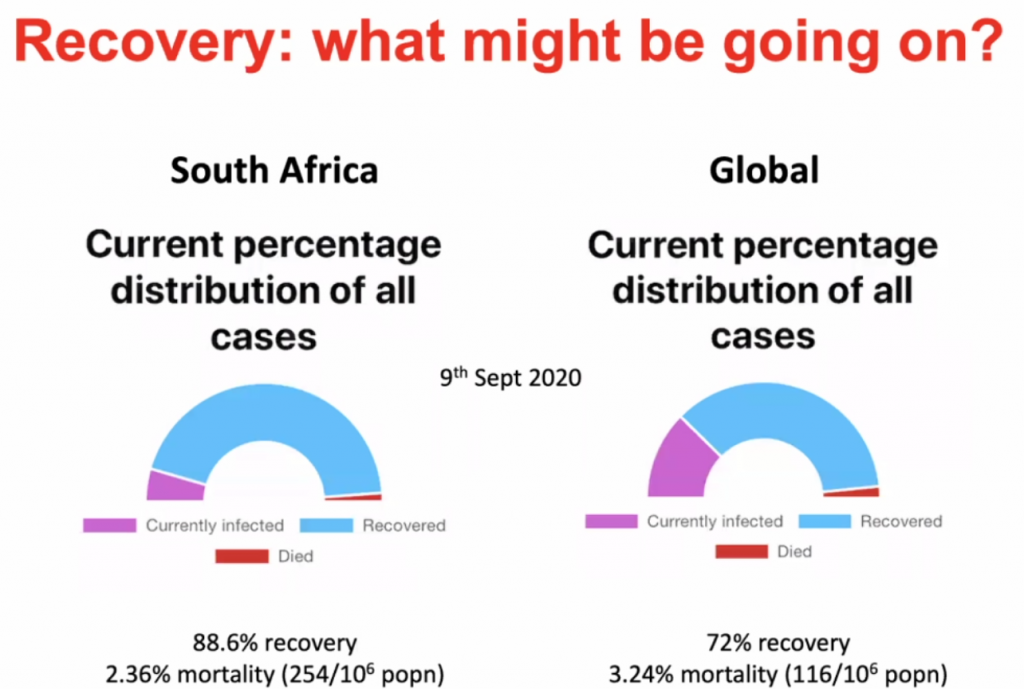
- What happens to people who progress to severe COVID-19?
- What might be happening in SARS-CoV-2 infected people who remain asymtomatic, have few symptoms and recover?
Internal : External world
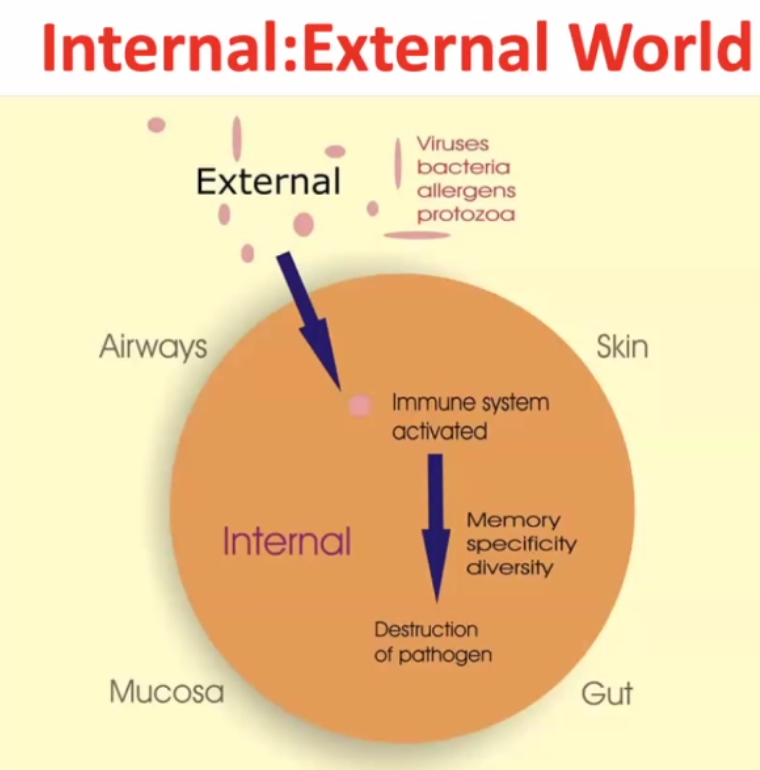
~99% of time the pathogen gets destructed, but the pathogen may survive in rare cases.
2 arms of immune responses:
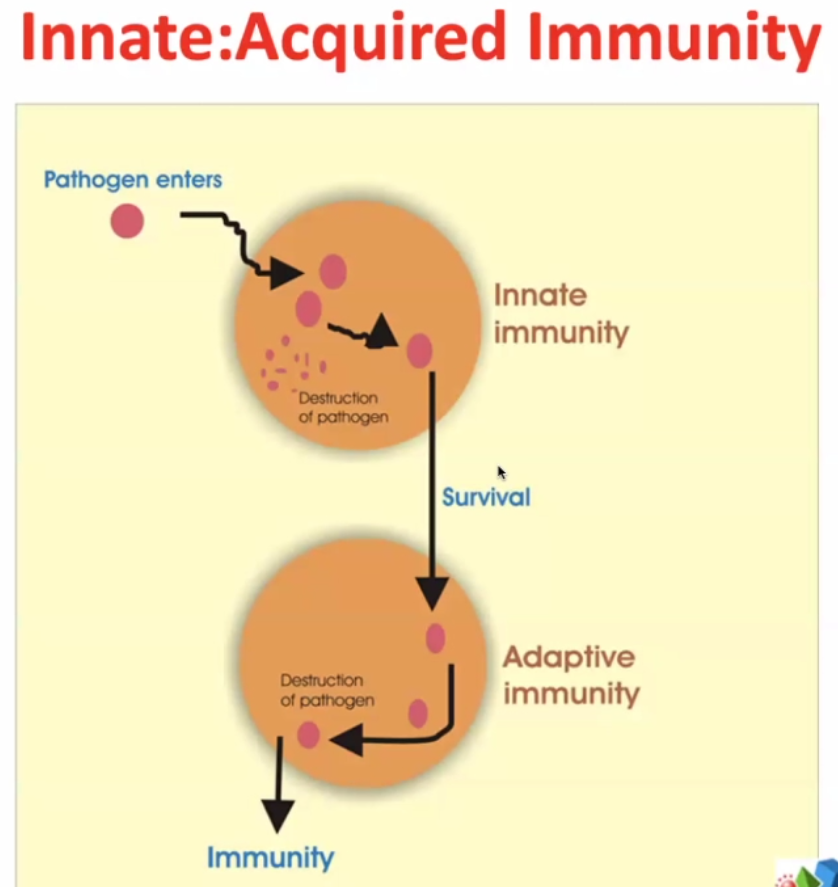
Innate – evolutionary response – very rapid – elements of innate immunity are found in bacteria, plants, lower vertebrates, squids, fish etc.
Some pathogens survive ->
Adaptive immunity – much more targeted / focussed. The immune system targets more specifically the pathogens which survive the innate immunity.
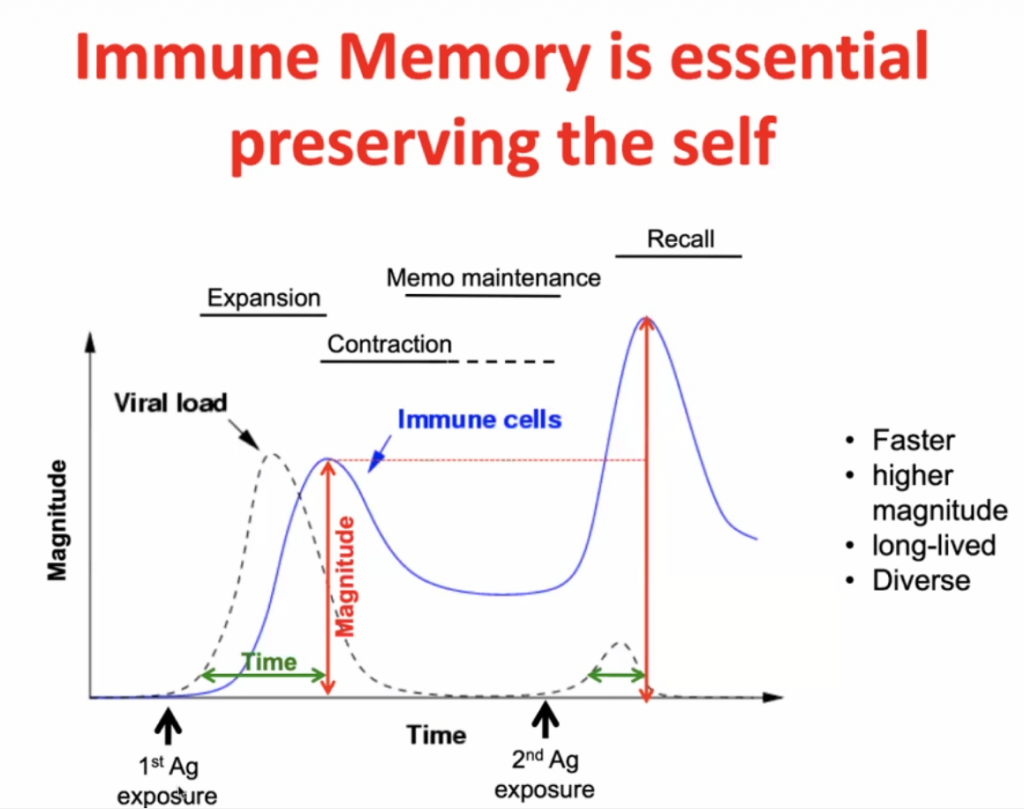
Infection initially -> expansion (peak after maximal viral load) -> contraction with some residual immunity (Memo Maintenance) -> with secondary response (Recall) there is a more rapid expansion (and higher peak) of the specific immunity.
Immune regulation:
Predisposed conditions: DM, HPT, Obesity, would make an individual highly susceptible to inflammation due to in imbalance of Inflammation vs. Tolerance, see below.
The Yin Yang of immunology:
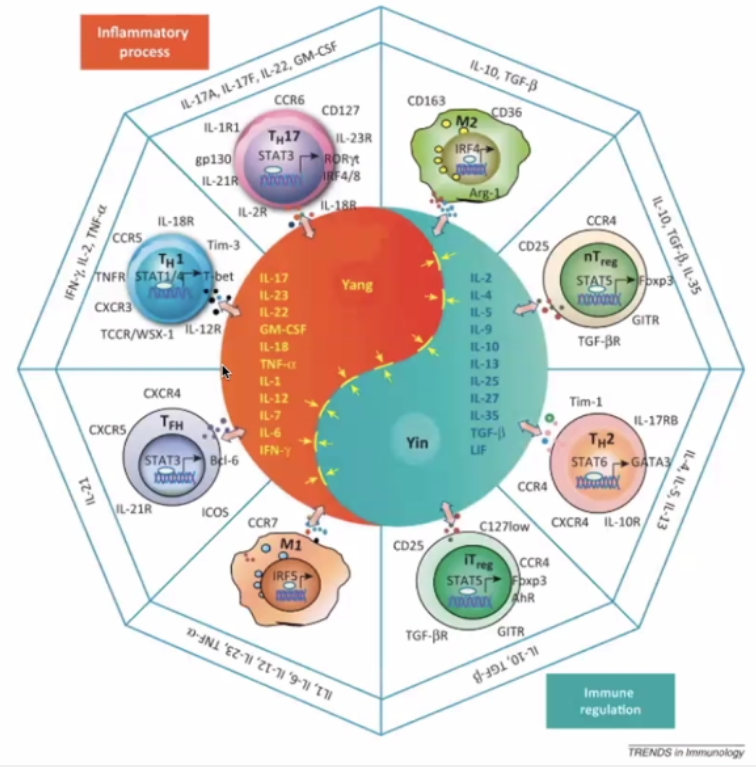
Pro-inflammatory (Orange)
TH17 – inflammatory cells secreting the “calling signals” for leucocytes.
TH1 – secreting IFN gamma; IL-2 ; TNF-alpha – cytokines causing inflammation
Macrophage – presents antigens – in lymph nodes and germinal centres
T-Helper cells T-FH
Immune Regulation (Blue)
TH2 – hand in hand with TH1 (opposite)
Regulatory cells (nT and iT regulatory cells)
Actual pathogen is not causing disease – but the immune response – thus this is what should be focussed on to treat the disease.
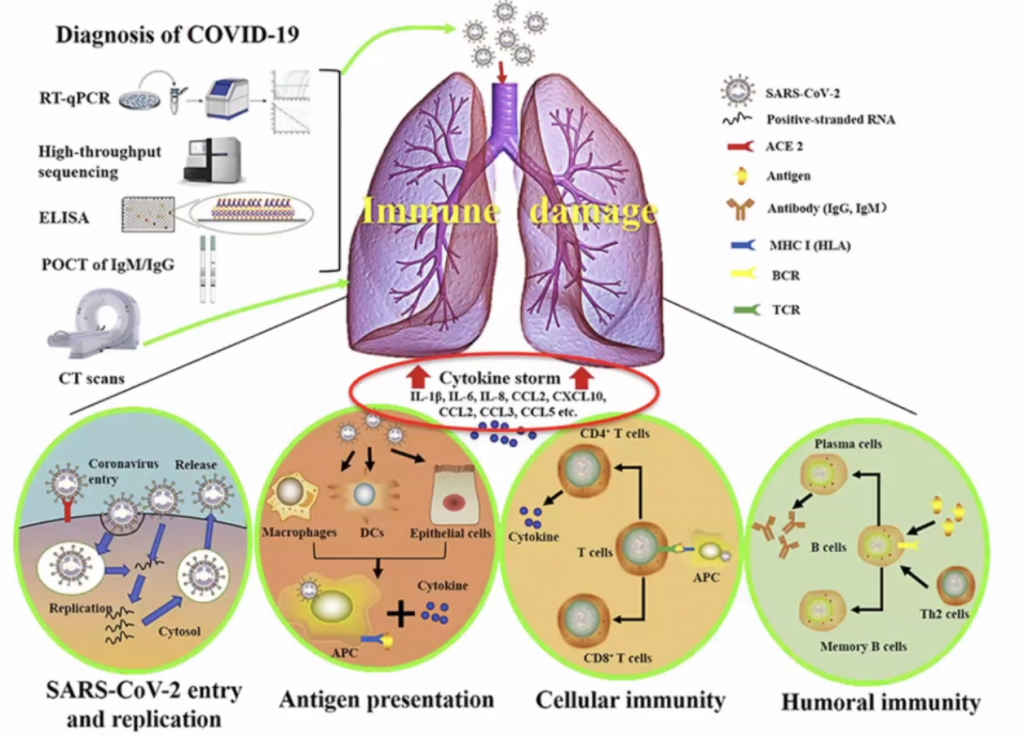
CCL’s allow leucocytes to migrate, hence in a cytokine storm, with high level of migration, the leucocytes causes severe local inflammation due to migration of leucocytes to local sites.
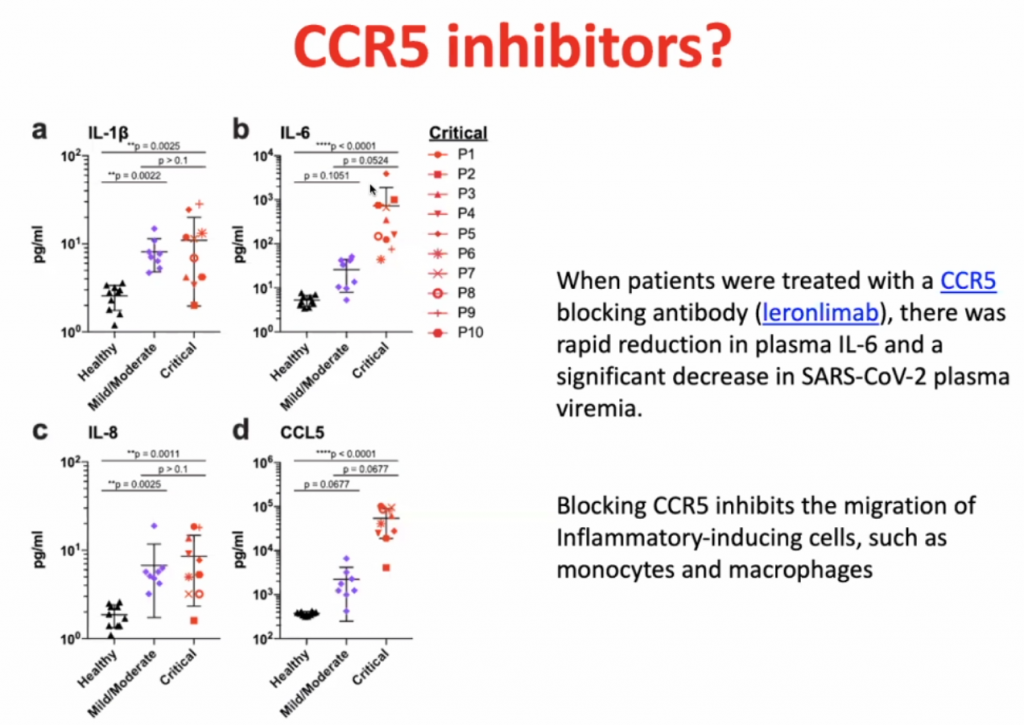
Dexamethasone is not so much an inhibitor of CCR5, but it prevents the hyperinflammation by inhibiting the majority of the inflammatory pathway.
CD8 cells
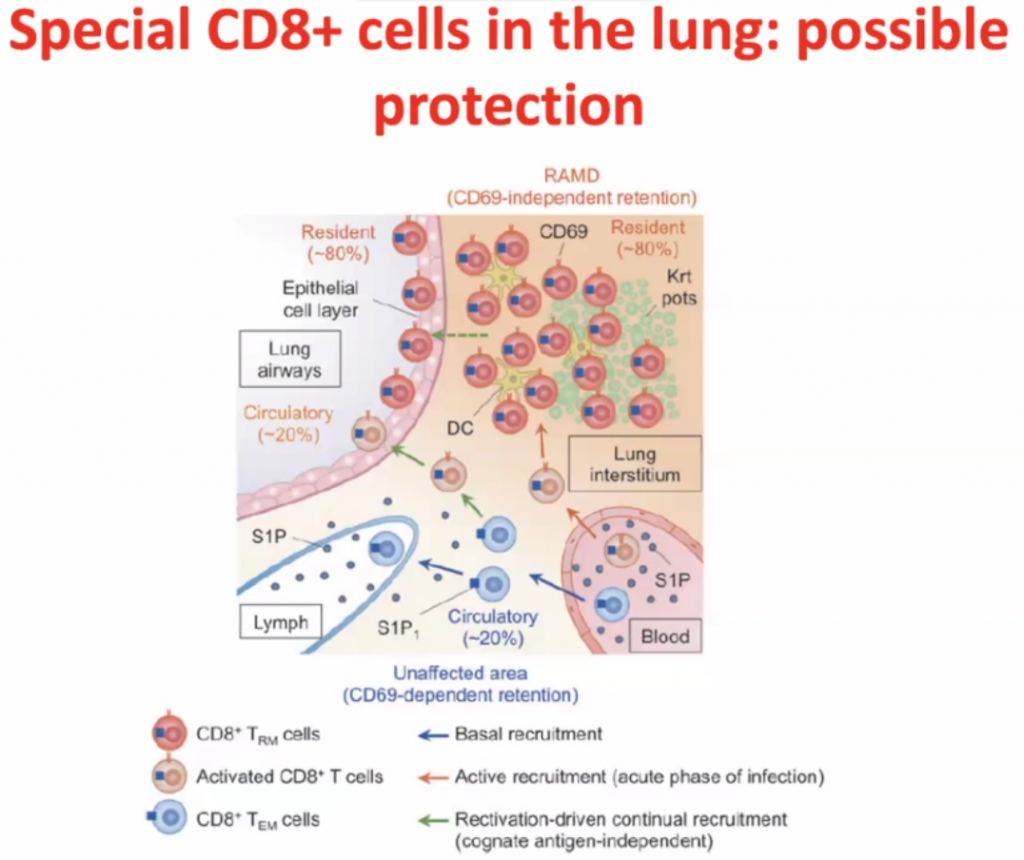
Within interstisium, the CD8 cells are present and
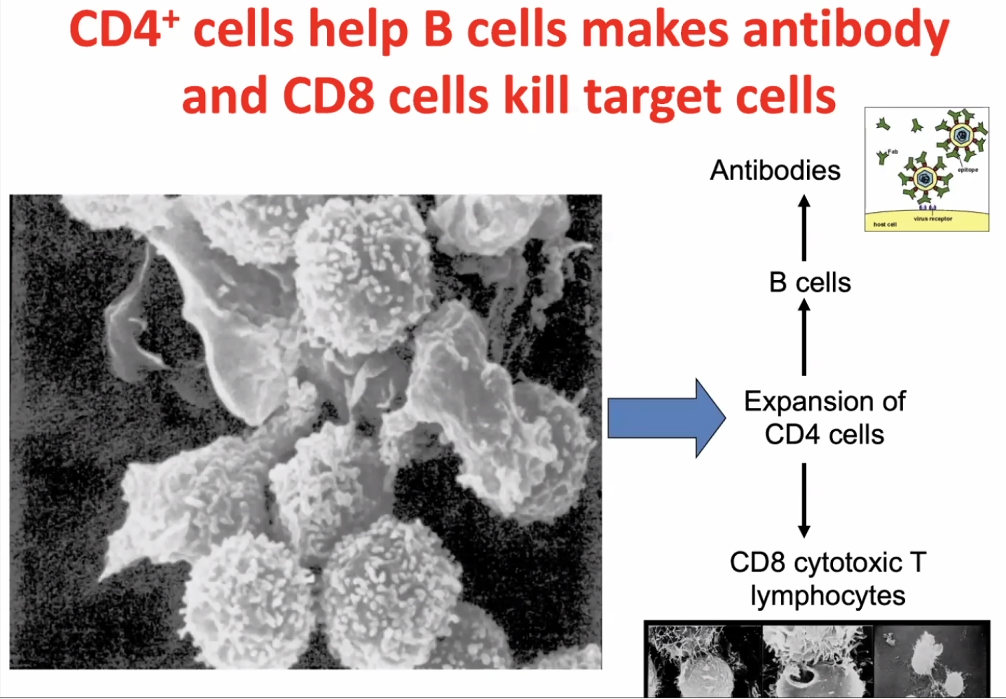
CD4 cells activates CD8 cells, hence called T-helper cells.