A case of amenorrhoea in a 17-year old female
| HOSP # | MRN94883340 | WARD | Paeds Endocrine Clinic |
| CONSULTANT | Jody Rusch / Ariane Spitaels | DOB/AGE | 17 year female |
Abnormal Result
Prolactin 51.1 ug/L
Monomeric Prolactin 36.2 ug/L
Presenting Complaint
Amenorrhoea (more details unknown)
History
The patient presented with a tempoparietal tumour and had received two episodes of radiotherapy – was asked by the oncologists to be reviewed by the Endocrinologists.
Mother stopped epilim (reason unknown)
Patient currently has amenorrhoea (unknown whether it is primary or secondary)
Examination
Residual right hemiplegia
Unfortunately no other facts about the physical examination are known
Laboratory Investigations
- Normal TFT:
- TSH 1.7 mIU/L (0.51 – 4.3)
- Free T4 16.2 (12.6 – 21.0)
- Cort 11am 330 nmol/L
- FSH 3.8 IU/L
- LH 2.4 IU/L
- E3 106 pmol/L
- Prol 51.1 ug/L
- Monomeric Prolactin 36.2 ug/L
- Recovery: 70.8%
Other Investigations
Proposed investigations:
- Pregnancy test (most common cause of amenorrhoea)
- Ovarian ultrasound to exclude early-onset PCOS (which may become a diagnosis of exclusion)
- History about prior amenorrhoea
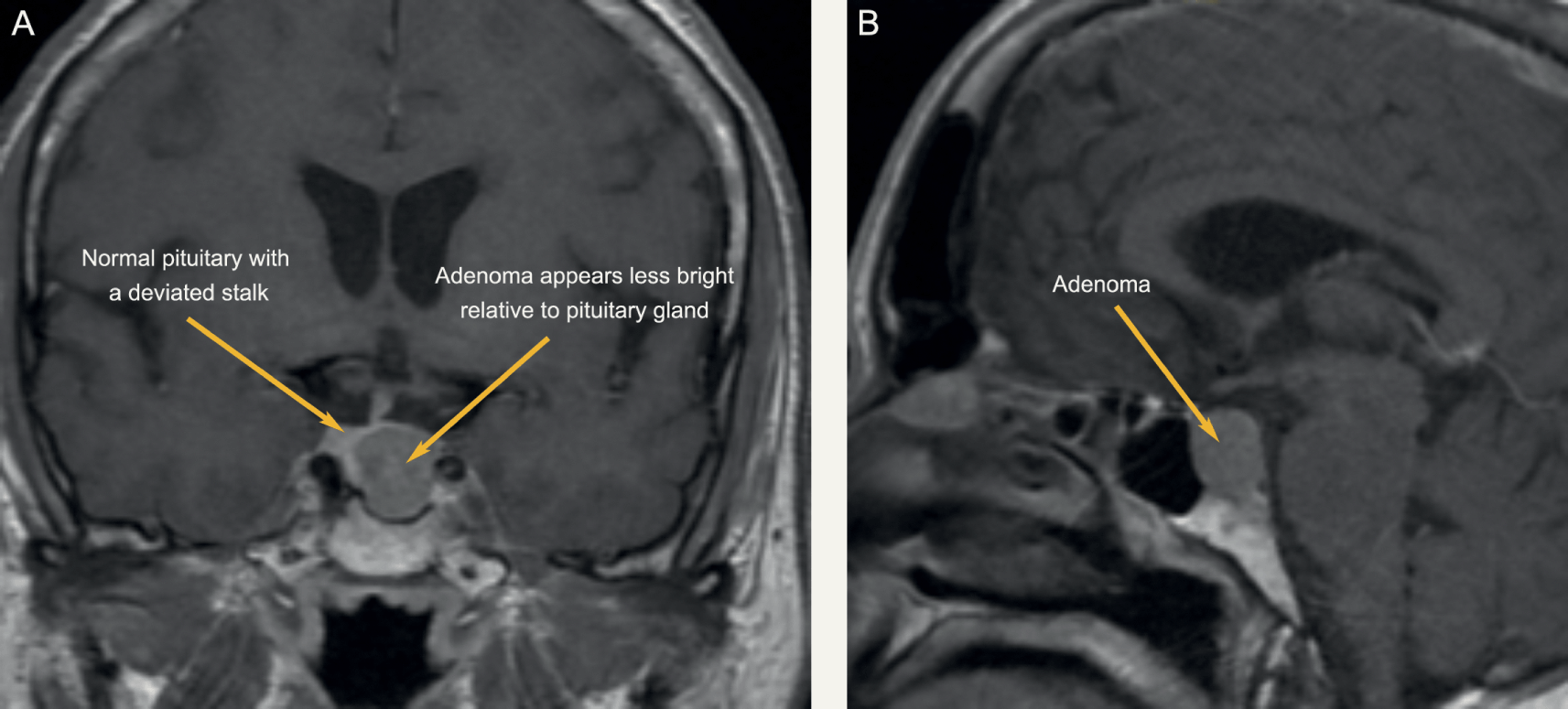
- Brain MRI to visualize pathology in the cranium
Final Diagnosis
Hyperprolactinemia – likely causing amenorrhoea – cause yet to be determined
Take Home Message
Hyperprolactinemia is perhaps one of the most common problems in clinical endocrinology. It relates with various aetiologies (see below), the clarification of which requires careful history taking and clinical assessment. Analytical issues (presence of macroprolactin or of the hook effect) need to be taken into account when interpreting the prolactin values. Medications and sellar/parasellar masses (prolactin secreting or acting through “stalk effect”) are the most common causes of pathological hyperprolactinaemia. Hypogonadism and galactorrhoea are well-recognized manifestations of prolactin excess, although its implications on bone health, metabolism and immune system are also expanding. Treatment mainly aims at restoration and maintenance of normal gonadal function/fertility, and prevention of osteoporosis; further specific management strategies depend on the underlying cause.
The main physiological causes of hyperprolactinemia:
- Ovulation
- Pregnancy
- Breastfeeding
- Stress
- Exercise
- Nipple stimulation or chest wall injury
Pathological
- Prolactin-secreting pituitary adenoma
- “Stalk-effect” from sellar / parasellar lesions
- Renal failure
- Liver cirrhosis
- Primary hypothyroidism
- Polycystic Ovarian Syndrome
- Seizures
Pharmacological
- Antipsychotics / neuroleptics
- Antidepressants
- Antiemetics
- Opioids
- Antihypertensives
It is clear in this case that the history is quite important in any patient in whom hyperprolactinemia is detected, since a vast array of causes exist.
For an excellent review on prolactin: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6947286/
For another case of high prolactin see: