Methylmalonic acidemia
| HOSP # | MRN123332237 | WARD | |
| CONSULTANT | Prof. George van der Watt | DOB/AGE | 5 day neonate |
Abnormal Result
Grossly increased Methylmalonic acid on urine organic acid analysis
Presenting Complaint
The baby presented as a 1 day neonate at the pediatric OPD with seizures and admitted to ICU.
History
The baby was discharged being normal after birth via a normal vaginal delivery. 24 hours later was brought to the hospital with seizures
Examination
Upon admission the neonate was encephalopathic with uncontrollable seizures.
Laboratory Investigations
| Test | Result (mmol/L) |
| Na | 142 |
| K | 5,8 |
| Cl | 108 |
| Bicarb | 12 L |
| Anion gap | 28 H |
| Urea | 16,3 H |
| Creat | 167 H (umol/L) |
Other Investigations
Ammonia in this child was >600 umol/L according to the clinician.
The child was managed as a possible urea cycle defect:
Glucose infusion, preventing catabolism, infusion of vitamins (co-factors). It is unknown whether specifically Vitamin B12 was given as well. Child likely had persistent lactatemia, also evidenced by the high lactate peak in the urine organic acid profile.
The neonate demised after 4 days in the ICU.
Urine organic acid analysis (unfortunately only analysed 2 weeks after demise) demonstrated increased levels of methylmalonic acid, 3-OH propionate, lactate, methylcitrate and a C5 dicarboxylic acid (likely glutarate).

Final Diagnosis
Methylmalonic aciduria
Take Home Message
There are a range of genetic defects causing an increase in Methylmalonic aciduria, but this case likely is
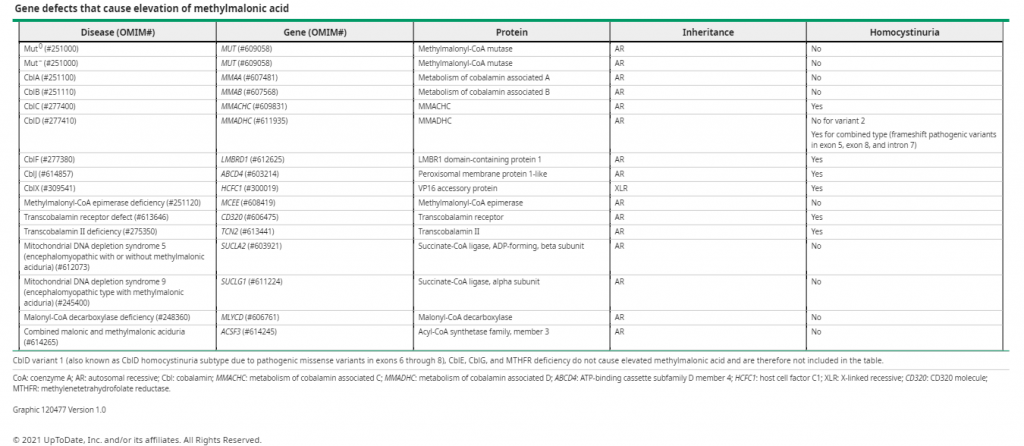
Patients presenting with ketosis, acidosis, and hyperammonemia may have methylmalonic acidemia or another organic acidemia. Evaluation of plasma acylcarnitines and urine organic acids can help to make the diagnosis. Organic acidemias may have a similar presentation, although patients with propionic acidemia may have more severe hyperammonemia than patients with MMA.
Other inherited metabolic disorders that cause elevated serum methylmalonic acid include combined malonic and methylmalonic aciduria, mitochondrial depletion syndrome due to autosomal-recessive pathogenic variants in SUCLA2 or SUCLG1, and also vitamin B12 deficiency.