Hyperaldosteronism
| HOSP # | WARD | Murraysburg Hospital, Female Ward | |
| CONSULTANT | DOB/AGE | 51 y female |
Abnormal Result
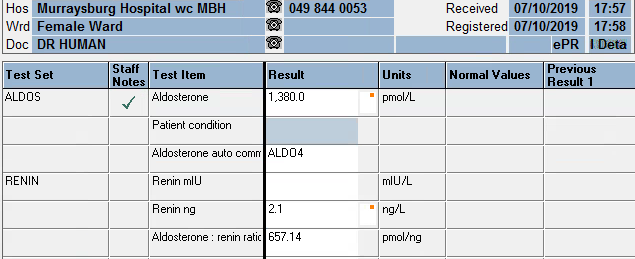
Aldosterone: 1380 pmol/L
Renin: 2.1 ng/L
Aldosterone: Renin ratio: 657.14 pmol/ng
Presenting Complaint
Uncontrolled Hypertension, unresolved on maximum dose of 3 antihypertensives.
History



Examination
Laboratory Investigations
Other Investigations
Urine electrolytes

Serum Results
| Date | Sodium mmol/L | Potassium mmol/L | eGFR ml/min | GGT U/L | Chol mmol/L | TSH mIU/L | T4 pmol/L | FreeT3 pmol/L | Cort nmol/L |
| 21/04/2015 | 2,8 | >60 | 5,07 | ||||||
| 30/11/2015 | 3,8 | >60 | 4,53 | ||||||
| 15/11/2016 | >60 | 4,04 | |||||||
| 20/03/2017 | >60 | 4,36 | |||||||
| 05/06/2018 | 144 | 3,4 | 56 | 4,39 | 1,79 | 11,9 | 5 | 394 | |
| 20/08/2018 | 131 | 4,6 | 42 | ||||||
| 21/08/2018 | |||||||||
| 24/08/2018 | |||||||||
| 26/08/2018 | |||||||||
| 26/08/2018 | |||||||||
| 26/09/2019 | 139 | 2,4 | 45 | 0.81 | |||||
| 27/09/2019 | 142 | 2,6 | 43 | ||||||
| 01/10/2019 | |||||||||
| 02/10/2019 | 139 | 2,9 | 40 | CEGK | |||||
| 03/10/2019 | |||||||||
| 07/10/2019 | 138 | 3,9 | 38 | ||||||
| 31/10/2019 | 139 | 1,9 | 30 | 28 |
Urine metanephrines
| Urine collection period | 24 h | Reference value |
| Urine volume | 3080 ml | |
| Ucreat | 2,2 mmol/L | |
| Umetadren | 160 nmol/L | |
| Unormetadren | 870 nmol/L | |
| dUmetadren | 493 nmol/24h | 152-913 |
| dUnormetadren | 2680 nmol/24h | 699-2643 |
| Umetadren:cr | 73 nmol/mmol creat | 17-91 |
| Unormetad:cr | 395 nmol/mmol creat | 75-309 |
Final Diagnosis
Primary hyperaldosteronism causing secondary hypertension with accompanying renal injury.
Take Home Messages
Reference Ranges for Aldosterone:
- Upright 70 – 1066 pmol/L
- Supine 49 – 643 pmol/L
Screening for primary hyperaldosteronism: most sensitive when >350 pmol/L
Reference Ranges for Renin:
- Upright: 2.7 – 27.7 ng/L
- Supine: 1.7 – 23.9 ng/L
Beta-blockers suppress renin levels and should be stopped 2 weeks before testing.
Aldosterone: Renin Ratio:
Most sensitive when the ratio is >118 pmol/ng.
Effects of hyperaldosteronism
- One’s expectation is a high serum sodium, but since it normalizes with an increase in fluid volume, hence hypertension as in this case, there is normal sodium.
- Low serum potassium due to loss in urine, although this can also be normal.
- Increased urine potassium concentration (>30 mmol/L) in a random urine specimen suggests increased mineralocorticoid effect.
- The renin:aldosterone ratio is used to compensate for the increase in aldosterone which is caused by an increase in renin (for instance which is caused by hypovolemia or low blood pressure).
- Some studies recently published are suggesting that the prevalence of hyperaldosteronism are significantly more than was (and is) thought, and hence urinary (24 hour) aldosterone measurement may be more accurate to screen for hyperaldosteronism. The authors of recent estimates of the prevalence of hyperaldosteronism are of opinion that hyperaldosteronism may be the cause of around 10% of unexplained “essential” hypertensives (see attached articles).