Thyroid Carcinoma
| HOSP # | WARD | Nuclear Medicine | |
| CONSULTANT | DOB/AGE | 62 y Female |
Abnormal Result
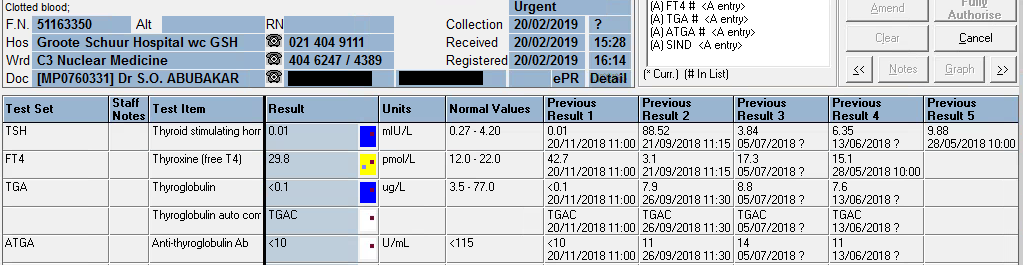
Thyroglobulin value of <0.1 ug/L upon signing results out.
Presenting Complaint
Patient presented with a neck “swelling” in October 2016. Systemic complaints were not inquired, but none was reported.
History
TFT: euthyroid since presentation when the thyroid functions were first tested in 2016.
Examination
A solitary thyroid nodule was found in the neck, moving with swallowing.
Laboratory Investigations
TFT: euthyroid upon presentation, which is clear from the table below.
| 07/11/2019 | 08/08/2019 | 21/06/2019 | 20/02/2019 | 20/11/2018 | 26/09/2018 | 21/09/2018 | 05/07/2018 | 13/06/2018 | 29/05/2018 | 07/05/2018 | 08/01/2018 | 05/04/2017 | 26/10/2016 | |
| TSH | δ- 1,49 | δ- 7,07 H | δ+62,97 H | 0.01 L | δ- 0.01 L | δ+88,52 H | 3,84 | 6,35 H | δ+ 9,88 H | 2,86 | 4,05 | δ+ 3,26 | 1,62 | |
| Free T4 | 21,4 | δ+ 22,3 H | δ- 3.0 L | δ- 29,8 H | δ+ 42,7 H | δ- 3,1 L | 17,3 | CEGK | 15,1 | δ+ 14,9 | 12 | |||
| Free T3 | 4,8 | |||||||||||||
| Thyroglobulin (3.5-77.0 ug/L) | <0.1 L | <0.1 L | 0.1 L | <0.1 L | δ- <0.1 L | 7,9 | 8,8 | 7,6 | ||||||
| Anti-thyroglobulin Ab (<115 U/ml) | <10 | <10 | <10 | <10 | <10 | 11 | 14 | 11 |
From results above it can be seen that the patient was euthyroid upon presentation (in 2016 and later until excision – highlighted in bold)
Hemithyroidectomy was done in May 2018, and another hemithyroidectomy in September 2018, thus the thyroglobulin after the first and second surgery was still detectable, but absent after September 2018.
Other Investigations
Ultrasound upon first presentation was indicative of a “suspicious nodule” in the thyroid gland.
Final Diagnosis
PATHOLOGICAL DIAGNOSIS – excision biopsy of nodule (17/01/2018)
Specimen A:
Right lobe of thyroid, hemithryoidectomy:
Encapsulated follicular variant of papillary thyroid carcinoma
Specimen B:
Right cervical lymph node (Level VI), biopsy:
Negative for malignancy (0/1)
PATHOLOGICAL DIAGNOSIS – left thyroid lobectomy (11/05/2018):
Left lobe of thyroid, excision: Negative for malignancy
PATHOLOGICAL DIAGNOSIS:
Right thyroid, lobectomy: Negative for malignancy (05/09/2018):
Take Home Messages
- Thyroglobulin level is directly proportional to thyroid tissue present in vivo, hence is a useful tumour marker for thyroid cancer.
- Anti-thyroglobulin antibody level is tested with Thyroglobulin to exclude false low values of thyroglobulin. If Anti-thyroglobulin Ab levels are increased with a decreased thyroglobulin level, the decrease in tumour marker is likely due to immunological clearance of the thyroglobulin and the result is hence likely false. This is the reason for the following canned text in TrakCare when the thyroglobulin level measures low:
The presence of thyroglobulin antibodies may interfere with the
thyroglobulin assay. The result of this test must be treated with reserve
if the patient has a positive thyroglobulin antibody test.TrakCare canned text for low thyroglobulin
- Upon total removal of the thyroid, thyroid replacement therapy is necessary, preferably slightly hyperthyroid levels to suppress TSH, and hence prevent tumour growth, as is also evidenced by this patient’s TSH and free T4 results.
- As with most other tumour markers, thyroglobulin should be used for follow-up as a proxy of tumour size or regression.