Possible Heterophile antibodies
| HOSP # | MRN77113313 | WARD | Endocrinology OPD |
| CONSULTANT | Dr. Jody Rusch / Dr. Khalid Aligail | DOB/AGE | 21y Female |
Abnormal Result
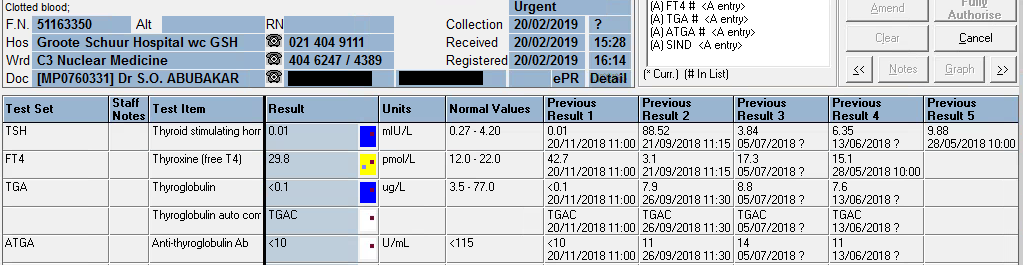
The TSH stayed elevated on our assay (Roche Cobas 6000) with a high-normal free T4.
Presenting Complaint
The patient was seen at the endocrinology OPD for follow-up of her thyroid function tests and review of medications. No acute complaints were noted, but some interesting thyroid function results became known.
History
Previous multinodular goiter with thyrotoxicosis. Had a complete thyroidectomy March-May 2020.
History of asthma, exema and “other allergies”.
Current dose of eltroxin = 1.6 ug/kg ~ 100ug/day PO. The patient (and doctor) declares good compliance to Rx.
Examination
Patient did not have any signs or symptoms of hypo or hyperthyroidism according to the endocrinologist.
Laboratory Investigations
| Date | 03/05/2021 | 26/04/2021 | 23/02/2021 | 23/10/2020 | 27/08/2020 | 08/05/2020 | 09/03/2020 |
| TSH (uIU/mL) (0.27 – 4.2) | •15,17 H | 18,54 H | 13.10 H | 21,61 H | 32,19 H | δ+>100.00 H | 7,72 H |
| Free T4 (pM) (12.0-22.0) | 17,8 | 17,7 | 18,3 | δ+ 16.0 | 11,8 L | δ- 9,7 L | δ+ 13,8 |
| Free T3 (pM) (3.1 – 6.8) | 4,3 | 4,2 |
The TSH seems to have stayed elevated on our assay (Roche Cobas 6000) with a high-normal free T4. The free T3 is normal (which I advised should be measured to assess conversion between the hormones). I also sent the sample to Green Point Laboratory where a Beckman DXi analyser is used with a different antibody set of reagents and a different reference range.
| Date | 03/05/2021 |
| TSH (uIU/mL) | 15.4 (0.38-5.33) |
| Free T4 (pM) | 13.6 (7.86-14.41) |
| Free T3 (pM) | 4.3 (3.8-6.0) |
Other Investigations
Auto-immune markers have been requested, since the patient was having prolonged iron deficiency, becoming anaemic, and the clincian raised a suspician of likely celiac disease.
Final Diagnosis
The diagnosis is still unsure, but the likely differential diagnosis is:
- Decrease in deiodinase activity due to some reason – there are many causes.
- Decrease in absorbtion of Levothyroxine
Take Home Message
Interference in thyroid function tests are commonly enquired about, especially by endocrinologists. This represents a big portion of our non-routine work and often quite a portion of time is spent on education of clinicians who do not necessarily have a laboratory background. Often, esoteric tests are requested which may not be warranted by the clinical scenario.
This case demonstrates a query raised by a clinician about possible interference in the TFT’s which is warranted. It is important to rule out as best one can, interference in the laboratory assay.
Various ways of determining whether interference is the culprit are:
- Dilution of the sample (in assays where the sample may be diluted – unsuitable for free-T4 as dilution will affect the “free” portion of hormone)
- Running the test on another methodology
- Running the test on another analyzer of the same methodology, but with slight differences, such as a different manufacturer of detection antibodies (e.g. Roche vs. Abbott vs. Siemens vs. Beckman vs. Ortho)
- Precipitating the antibodies e.g. desalting, or PEG-precipitation.
- Binding the antibodies, e.g. protein G or Protein A
- Using of “blocking tubes” which is a proprietary blood collection tube to bind antibodies