A case of hypertriglyceridemia with Diabetes mellitus
| HOSP # | WARD | Albow Gardens Clinic | |
| CONSULTANT | Prof. David Marais | DOB/AGE | 31 y Male |
Abnormal Result
31 y/o Male
Presenting Complaint
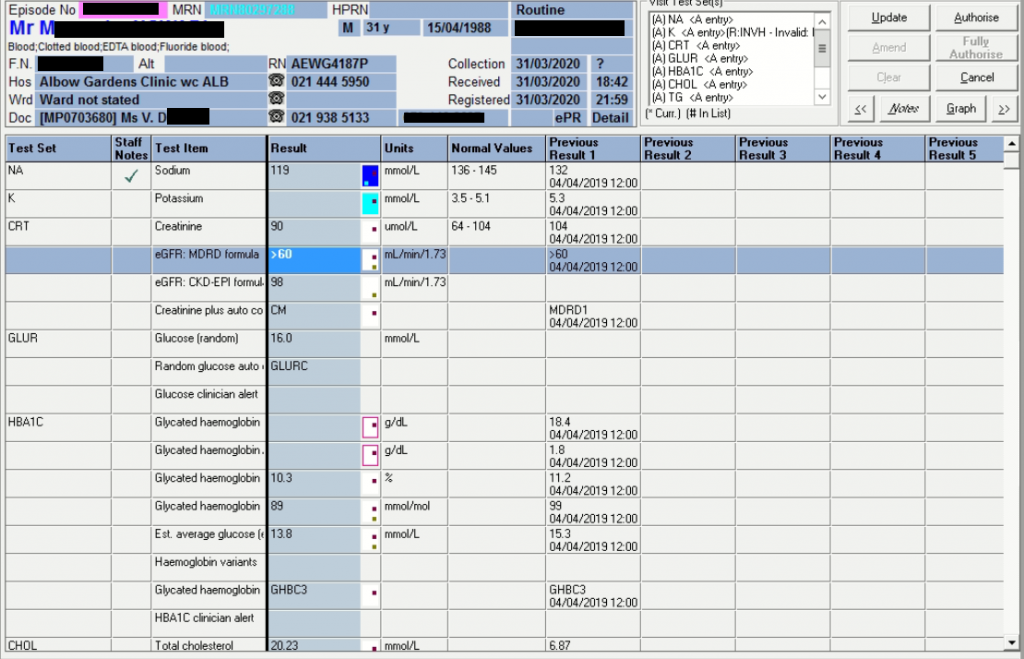
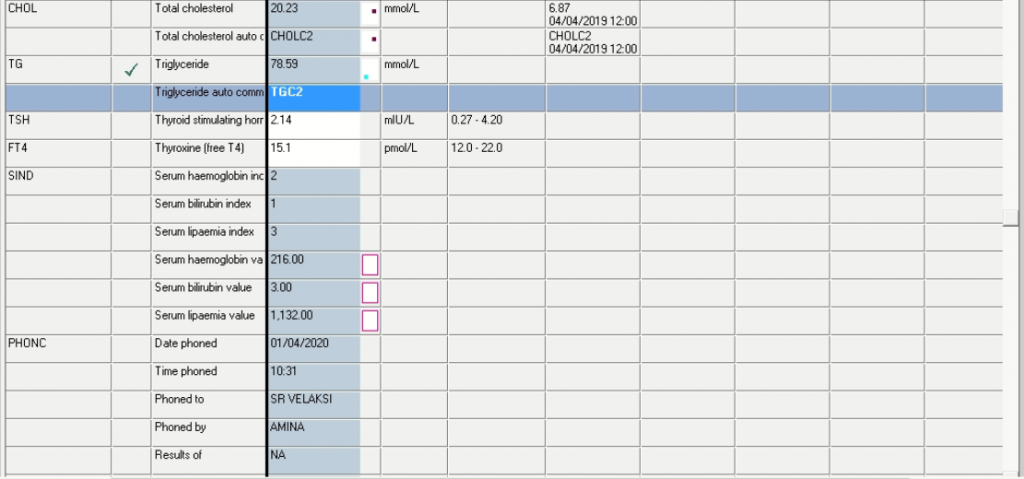
Triglycerides of 78.59 mmol/L
Lipaemia index 3 (value of 1132)
It is likely that the results as set out above was due to a routine follow-up, but unfortunately little clinical information was given by the clinician.
History
The patient is hypertensive and diabetic on treatment since 2018. No other clinical information was given and the drug list was not supplied.
Examination
N/A – No signs and symptoms obtained.
Laboratory Investigations
Other Investigations
We would have loved to do lipid electrophoresis and see better investigations into the cause of the diabetes, but at the time of writing, 14/05/2020, the patient has unfortunately not had the opportunity to follow-up and it can unfortunately not be shown.
In an adult diabetic one would however expect the lipid electrophoresis to be that of a Fredrickson type V.

Hyperlipoproteinemia type V, also known as mixed hyperlipoproteinemia, familial or mixed hyperlipidemia, is very similar to type I, but with high VLDL in addition to chylomicrons.
It is also associated with glucose intolerance and hyperuricemia.
Final Diagnosis
Considering most factors known, and as explained via feedback from Prof. Marais below, diabetes is likely type 2 related to insulin resistance. One should also consider metabolic errors such as glucokinase deficiency causing MODY. Other causes, but unlikely, are endocrine pancreatic insufficiency which could include mitochondrial defects or herbicide-induced diabetes or (post-traumatic) excision of tail of pancreas. HbA1c shows prolonged exposure to high glucose concentrations: 10.3% and 11.2% the year before.
Take Home Message
The following were my thoughts on causality of the high triglycerides initially:
Increased intake:
- Overeating (unlikely for this high Triglyceride level), that is why one has lipoproteins – to keep the fat in the blood low and store the fat in liver and tissues.
- Excess alcohol consumption, but I’m also not sure (wasn’t sure) if excess alcohol will raise triglycerides this high – it likely may (after prof’s email I think this is very likely the main cause in this patient).
Increased production:
- Kidney failure (nephrotic syndrome) (Prot: Creat ratio will likely exclude this – if borderline, a protein electrophoresis can be done).
Decreased metabolism:
- Some forms of familial hyperlipidemia such as familial combined hyperlipidemia
- Lipoprotein lipase deficiency
- Lysosomal acid lipase deficiency (aka cholesteryl ester storage disease)
- Hypothyroidism (TFT’s normal in this patient though)
- SLE
- Glycogen storage disease type 1 –> NAFLD (non-alchoholic fatty liver disease)
Drugs:
- Isotretinoin, Thiazides,
- Apparently some HIV meds.
How to further test:
Lipid electrophoresis will delineate the Fredericksen Class.
Familial combined hyperlipidemia:
Lipid electrophoresis will show lipoproteinemia type IIB.
LPL deficiency:
Lab tests show massive accumulation of chylomicrons in the plasma and corresponding severe hypertriglyceridemia. Typically, the plasma in a fasting blood sample appears creamy (plasma lactescence).
The absence of secondary causes of severe hypertriglyceridemia (like e.g. diabetes, alcohol, estrogen-, glucocorticoid-, antidepressant- or isotretinoin-therapy, certain antihypertensive agents, and paraproteinemic disorders) increases the possibility of LPL deficiency. Also other loss-of-function mutations in genes that regulate catabolism of triglyceride-rich lipoproteins (like e.g. ApoC2, ApoA5, LMF-1, GPIHBP-1 and GPD1) should also be considered. (remember our case – I won’t mention her name though, patient’s name begins with a K… and ends with …ana).
The diagnosis of familial LPL deficiency is finally confirmed by detection of either homozygous or compound heterozygous pathogenic gene variants in LPL with either low or absent lipoprotein lipase enzyme activity (Jody and I have done this assay with Bharati and Prof once for above patient).
Lysosomal acid lipase deficiency (LAL-D) (aka cholesteryl ester storage disease) – Unlikely – would rather present earlier – the accumulation of fat in the walls of the gut in early onset disease leads to serious digestive problems including malabsorption, the gut fails to absorb nutrients and calories from food. Because of these digestive complications, affected infants usually fail to grow and presents with failure to thrive. As the disease progresses, it can cause life-threatening liver dysfunction or liver failure). Until 2015, apparently there was no treatment (not sure if this is true though), and very few infants with LAL-D survived beyond the first year of life.
I think the clinical presentation and examination and history is much needed before any further investigations are advised.
Also, one should appreciate the size difference which is partly responsible for the electrophoretic mobility of lipoproteins on a gel.

Feedback from Prof. David Marais:
Hi Dieter
Thanks for distributing the interesting case information. The patient is at very high risk of developing acute pancreatitis. Hopefully the medical officer will be able to get in touch with the patient and urgently:
- (1) control diabetes mellitus and
- (2) restrict dietary fat intake to 10g/d for a few days whereafter 30-40g/d.
- (3) restrict alcohol intake to preferably zero or certainly <20g/d.
- (4) prescribe fibrate.
- (5) Referral to the lipid clinic – unfortunately may take time owing to shut-down of out-patients clinics in the precautions against corona virus spread.
Such severe hyperTGaemia seen in the neonate, infant or child is most likely due to an error in the lipolytic system and all of these are recessively inherited. LPL deficiency is the commonest but there may also be apoCii, apoAv, GPIHBP1 or LMF1 deficiency. In adolescent and young adults the same causes apply but also auto-immune LPL inhibition. In these cases all the agarose gel electrophoresis for lipoprotein separation will display a type I pattern. The highest TG conc I have seen in a patient was 695mmol/L and at 6 weeks of age.
In adults the lipoprotein electrophoresis pattern will usually be a type V. Here, there is usually partial lipase deficiency (often polygenic heterozygotes of LPL system components) and a dietary or metabolic stress. Diet containing triglycerides in large amounts and alcohol. Metabolic stress is mostly diabetes with increased return of NEFA to the liver and export as VLDL. Occasionally, apoE2/2 status with impaired remnant clearance can have a backlogue effect to raise VLDL and chylomicrons. Rarely, in partial lipodystrophies the adipose tissue does not take up NEFA from LPL and the liver puts out more VLDL which competes with chylomicrons for lipolysis. Typically this is associated with diabetes as well. Significant hypothyroidism and renal impairment appear to be excluded as potential secondary causes.
The results indicate long-standing diabetes and hyperlipidaemia. There is likely pseudohyponatraemia. This is because the aqueous part of the aliquot for analysis can be significantly less than the whole volume. The response is to do highspeed or ultracentrifugation so that the lipid can float and the infranatant plasma can be best analysed. Obviously, the whole plasma should be first assayed (in dilution with saline) to be certain of the TG concentration. Alternatively, the lipid volume can be calculated by converting the mmol/L of TG + CE + phospholipid to mass/L and then using the specific gravity of 0.92 g/mL to obtain the volume correction. For practical purposes only the TG and cholesterol values may be used as we do not routinely measure the phosphatidyl choline. Average MW of TG =850da, of CE = 650da, of PL = 750da. Note that usually 70% of cholesterol is esterified. Cholesterol MW = 387da.
Per L, TG of 79mmol/L is 67g, CE of 14mmol/L is 9g, total lipid is 85g.
Each g being 1.09mL, makes this 92.4g/L or 9.24g/100mL. This means that the aqueous portion of the aliquot is about 10% too low. This makes the calculated Na+ concentration about 131mmol/L which is still not normal but certainly closer to the reference range. But the calculation is not highly accurate; partly because PL has not been taken into account; unesterified cholesterol is quantitatively less important.
Diabetes is likely type 2 related to insulin resistance but at this age and especially if dominantly inherited, consider metabolic errors in MODY such as glucokinase deficiency. Unlikely endocrine pancreatic insufficiency which could include mitochondrial defects or herbicide-induced diabetes or (post-traumatic) excision of tail of pancreas. Not certain if patient is on IV line that could provide lipid (Intralipid in parenteral nutrition) or glucose. Regardless, HbAic shows prolonged exposure to high glucose concentrations.
Regards
D
Professor Emeritus AD Marais
Chemical Pathology 6.33 Falmouth Building
University of Cape Town Health Sciences
Anzio Rd, Observatory, 7925
Cape Town, South Africa