A possible case of glycerokinase deficiency
| HOSP # | WARD | Ward B2 | |
| CONSULTANT | George van der Watt | DOB/AGE | 3 month |
Abnormal Result
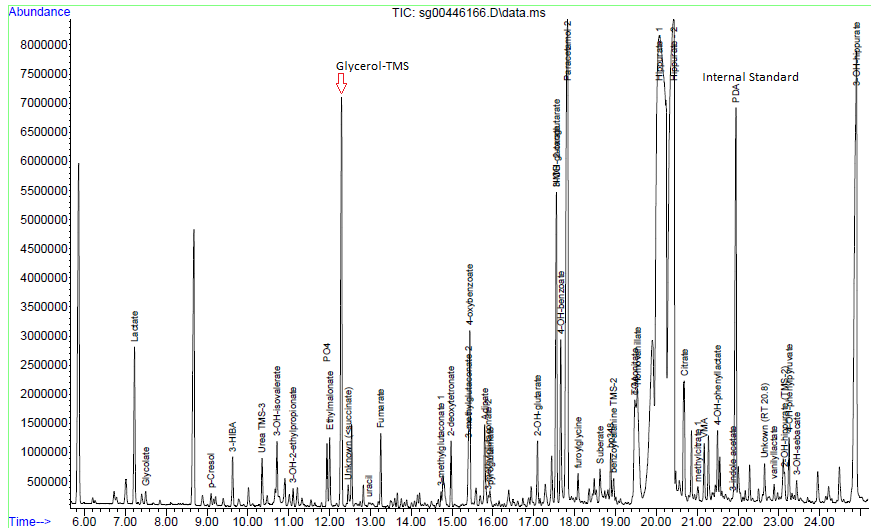
Glycerol which is significantly raised on urine organic acid analysis.



Presenting Complaint
Patient is a 3 month old male with signs and symptoms of sepsis.
History
Patient presented with significant failure to thrive.
Laboratory Investigations
Triglycerides : 4.47 mmol/L
Other Investigations
Faecal elastase 81 ug/g stool
Reference range (adults and children > 1 month):
- > 200 ug elastase/g stool: Normal exocrine pancreatic function
- 100-200 ug elastase/g stool: Moderate/mild pancreatic insufficiency
- < 100 ug elastase/g stool: Severe exocrine pancreatic insufficiency
These ranges apply to formed stool samples. Watery stool samples may yield spuriously low elastase results due to dilution, and a formed stool sample should be sent for re-analysis.
Final Diagnosis
Glycerol contamination of the skin – as excluded by the repeat analysis.
Take Home Message
- Glycerol (glycerine) is a common contaminant of urine organic acids due to being present in various skin products / creams. Contamination can be eliminated by thorough cleaning of the perineum with normal saline or doing an “in-out” catheterization procedure for urine collection in neonates. Interestingly glycerol is also one of the main ingredients in KY jelly, a common lubricant use for catheterization.
- High glycerol in serum will present with a falsely high triglyceride level on most routine chemistry analysers due to the inherent enzymatic conversion of triglycerides to glycerol before further steps to measurement.

- Sepsis is more common than inherited metabolic diseases and so is pre-analytical caveats such as glycerol contamination of the perineal skin.
