Fluid Triglycerides
| HOSP # | WARD | Surgical ICU | |
| CONSULTANT | Dr. Heleen Vreede | DOB/AGE | 23y Female |

Abnormal Result
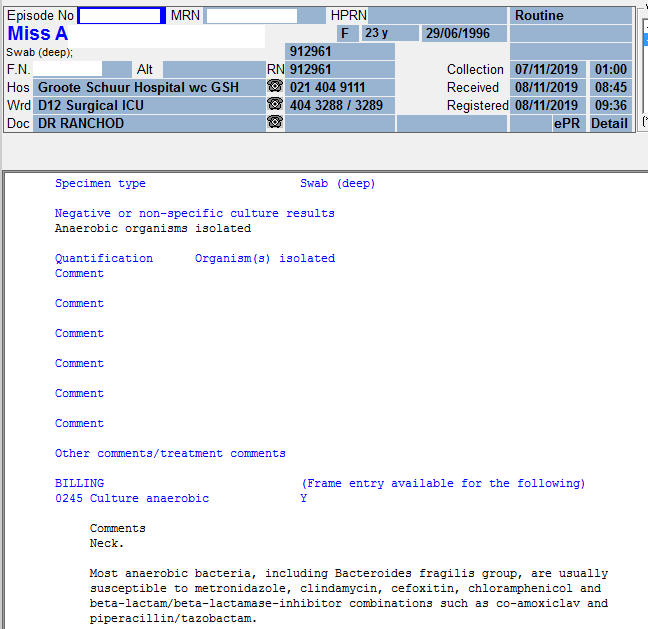
Fluid triglycerides were requested on three samples, without any clinical information.
Presenting Complaint
The laboratory history was explored, to find that the patient had three subsequent samplings daily from a pleural fluid cavity.
History
A month prior to presentation, the patient had a breached stillbirth.
The following was found on Histology:
EPISODE NUMBER: SA03381462 CLINICAL DETAILS: 23 year old female. G02 P2-1. VDRL: negative. Smoking: 8/day. Alcohol: none. HIV: negative. 750g breech stillbirth at 28/40. MACROSCOPY: The plate measures 130 x 100 x 30mm and weighs 196.8g. The membranes are complete without evidence of meconium staining. The cord measures 300mm in length with an average diameter of 15mm. Three umbilical vessels are identified with 3 twists per 100mm. The cord insertion is off-centre, 20mm from the plate margin. Congested blood vessels are identified on examination of the foetal surface. Cut-sections of the plate show: - Retroplacental clot. MICROSCOPY: General: Placental weight for gestational age is below the 10th percentile at 196.8g. Partial autolysis is present throughout the specimen. The umbilical cord and membranes: The umbilical cord contains two arteries and one vein. There is no evidence of vasculitis or funisitis. Wharton's jelly and membranes do not show meconium uptake. The amniocytes are intact and show no evidence of vacuolation or hyperplasia. Chorionic plate: The chorionic plate vessels are focally dilated. There is no evidence of chorioamnionitis. Villi and intervillous spaces: The stem villous vessels show partial obliteration as well as stromal sclerosis. Distal villous hypoplasia as well as accelerated villous maturation is seen. Intervillous thrombi are seen as well as intraparenchymal extension of the retroplacental haematoma. There is no evidence of infarction, villitis or intervillositis. Maternal surface: There is evidence of a large retroplacental haematoma. No chronic deciduitis or untransformed blood vessels are seen. PATHOLOGICAL DIAGNOSIS: Placenta, examination: Maternal vascular malperfusion. Retroplacental haematoma. Reported by: Dr M Du Toit
Clinicians were indeed querying a chylothorax. A thoracic duct injury was suspected.
Examination
Unfortunately little clinical information is known, as can be seen above. The following table shows the clinical info which has been captured on the respective episodes’ request forms:
Clinical history for episodes
< SA03215505 > ?UTI IN PREGNANCY
< SA03381462 > 03/10/2019 PLACENTA
< SA03466495 > 07/11/2019 MEDIASTINITIS
< SA03466500 > 08/11/2019 MEDIASTINITIS
< SA03466533 > 08/11/2019 MEDIASTINITIS
< SA03467168 > 08/11/2019 MEDIASTINITIS
< XC00366131 > ILLEG
< SA03467081 > ILLEGIBLE
< SA03469305 > NECK ABSCESS
< SA03469995 > ILLEGIBLE
< SA03472064 > MEDIASITINITIS
< SA03470738 > NECK ABSCESS
< SA03476491 > PUS FLUID + MEDIASTINITIS
< SA03476496 > PUS / FLUID + MEDIASTINITIS
< SA03476502 > PUS / FLUID + MEDIASTINITIS
< SA03476507 > PUS / FLUID + MEDIASTINITIS
< SA03489396 > ?CHYLOTHORAX
< SA03485823 > SEPSIS
< SA03491179 > NECK ABSCESS
< SA03493180 > Neck abscess with sepsis.
< SA03494446 > CVC TIP
< SA03509355 > LOOSE STOOLS
< SA03513657 > THORACIC SURGERY
< SA03531013 > MEDIASTINITISLaboratory Investigations

Other Investigations
Final Diagnosis
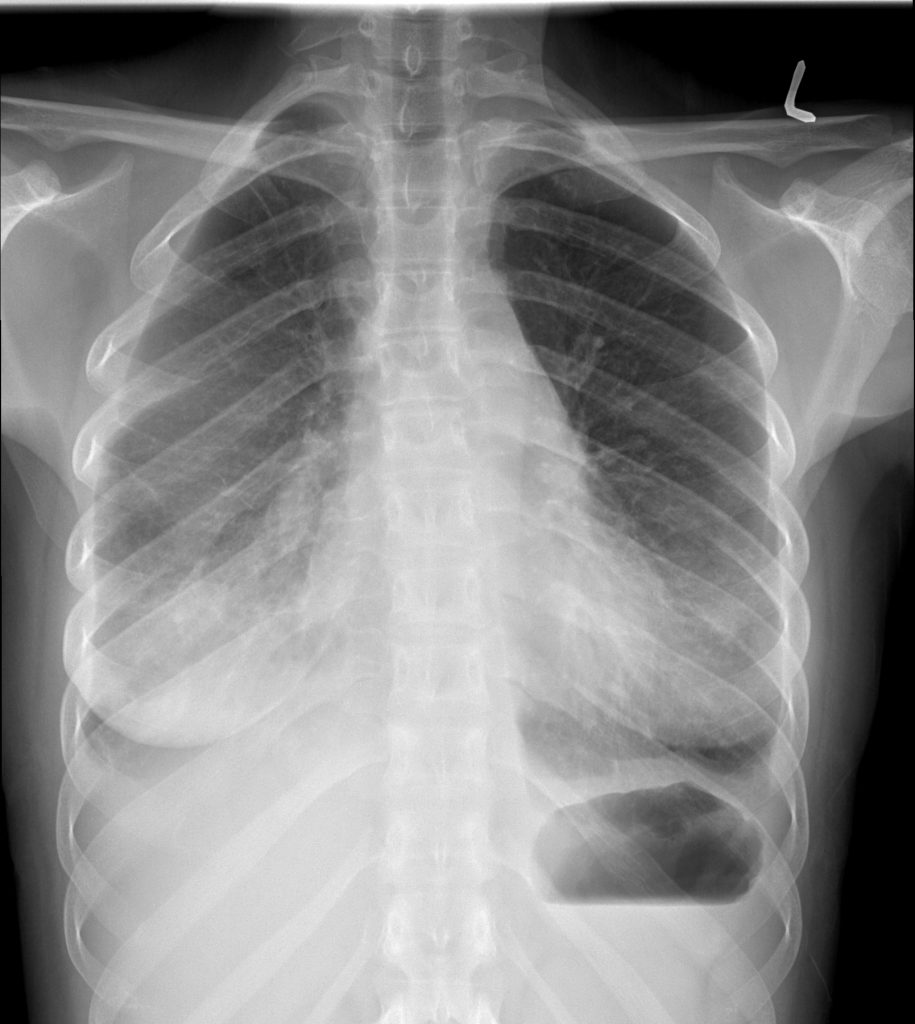
A pleural fluid triglyceride >1.24 is suggestive of chylothorax.
The additional finding of a thin white layer present on the top of the sample after centrifugation indicates the presence of chylomicrons in the sample, which further supports the diagnosis of chylothorax.








Take Home Messages
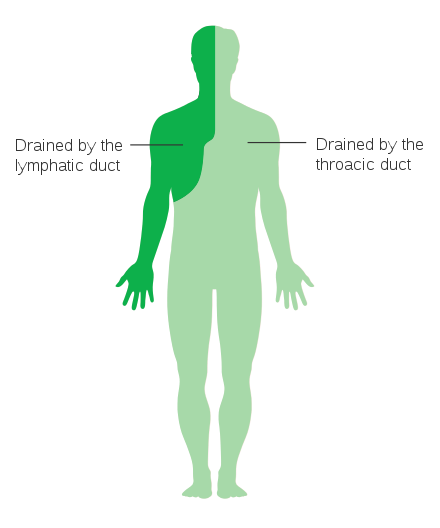
The primary role of the thoracic duct is to carry 60 – 70% of ingested fat at a concentration of 0.4 – 6 g/dl from the intestine to the circulatory system.
- Chyle contains large amounts of cholesterol, triglycerides, chylomicrons and fat soluble vitamins.
- Lymph is the other main constituent of chyle and is made up of
- immunoglobulins
- enzymes
- between 400 and 6800 white blood cells/ml, the majority of which are lymphocytes.
- Chyle transportation is maximal after a high fat meal and minimal with starvation where flow is reduced to almost a trickle.


Classically, a chyloma, a collection of chyle below the pleura develops when the thoracic duct first leaks. Although rarely detected, it manifests itself as a swelling in the supraclavicular fossa which may be associated with severe chest pain, dyspnoea and tachycardia.
Chylomas can also manifest themselves at other sites of the pleura without causing supraclavicular swelling. Eventually the chyloma bursts through the pleura where the chyle accumulates in the pleural space.
Very rarely, the chyle leak may lead to chylomediastinum or chylopericardium.

Roughly 2.4 l of chyle is transported through the lymphatic system every day.
Damage to, or rupture of the thoracic duct can give rise to a large and rapid accumulation of fluid in the pleural space.
Causes of chylothorax can be classified as follows:
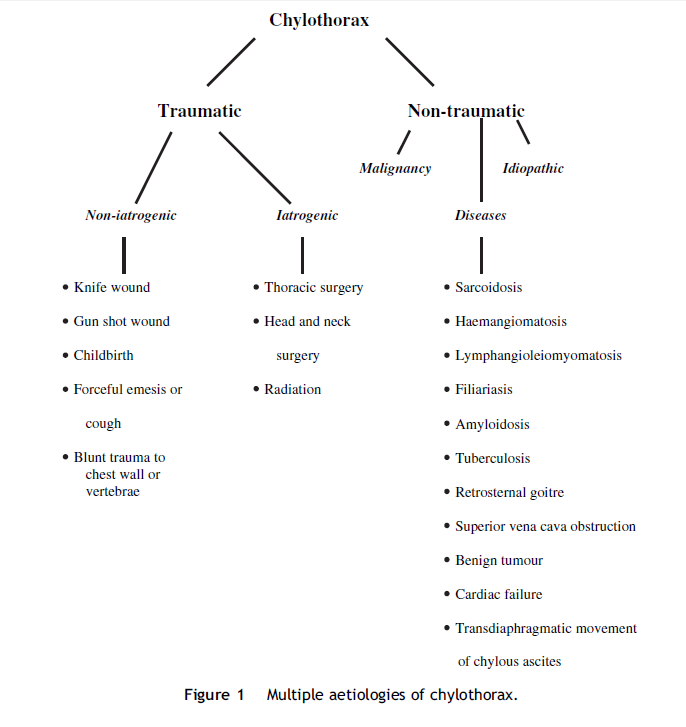
The theorized causes of chylothorax in this case could be one of the following:
- The breached stillbirth a month prior to presentation could have caused rupture of the thoracic duct due to increased pressure due to extreme valsalva. Could this be dormant for 1 month and then present with the neck abscess with an anaerobic infection? Could anaerobic bacterial transmission from the gut into a chylous cyst in the neck be the cause? It is however unlikely that delivery of a 750g fetus causes that much trauma.
- Iatrogenic chylothorax due to the thoracic surgery.
- Left-sided placement of a Central Venous Catheter during delivery of the stillbirth, which accidentally damaged the thoracic duct. The placement of the CVP could also have caused a pneumothorax with subsequent stretching and damage to the thoracic duct.
Remember Chylomicrons float!
